Privatization and Disinvestment - Meaning, Objectives, Advantages and Disadva...
Viral Infections of the Oral Cavity
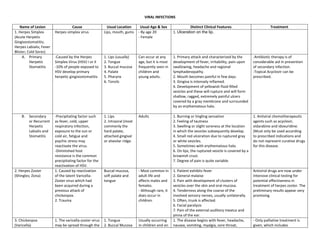
1. VIRAL INFECTIONS
Name of Lesion
1. Herpes Simplex
(Acute Herpetic
Gingivostomatitis;
Herpes Labialis; Fever
Blister; Cold Sores)
A. Primary
Herpetic
Stomatitis
B.
Secondary
or Recurrent
Herpetic
Labialis and
Stomatitis
2. Herpes Zoster
(Shingles; Zona)
3. Chickenpox
(Varicella)
Cause
Herpes simplex virus
Usual Location
Lips, mouth, gums
Usual Age & Sex
- By age 20
- Female
Distinct Clinical Features
1. Ulceration on the lip.
Treatment
-Caused by the Herpes
Simplex Virus (HSV) I or II
-10% of people exposed to
HSV develop primary
herpetic gingivostomatitis
1. Lips (usually)
2. Tongue
3. Buccal mucosa
4. Palate
5. Pharynx
6. Tonsils
Can occur at any
age, but it is most
frequently seen in
children and
young adults.
1. Primary attack and characterized by the
development of fever, irritability, pain upon
swallowing, headache and regional
lymphadenopathy.
2. Mouth becomes painful in few days.
3. Gingiva is intensely inflamed.
4. Development of yellowish fluid-filled
vesicles and these will rupture and will form
shallow, ragged, extremely painful ulcers
covered by a gray membrane and surrounded
by an erythematous halo.
-Antibiotic therapy is of
considerable aid in prevention
of secondary infection.
-Topical Acyclovir can be
prescribed.
-Precipitating factor such
as fever, cold, upper
respiratory infection,
exposure to the sun or
cold air, fatigue and
psychic stress may
reactivate the virus.
-Diminished host
resistance is the common
precipitating factor for the
reactivation of HSV.
1. Caused by reactivation
of the latent VaricellaZoster virus which had
been acquired during a
previous attack of
chickenpox.
2. Trauma
1. Lips
2. Intraoral (most
commonly the
hard palate,
attached gingival
or alveolar ridge.
Adults
1. Burning or tingling sensation
2. Feeling of tautness
3. Swelling or slight soreness at the location
in which the vesicles subsequently develop.
4. Small red ulceration due to ruptured gray
or white vesicles.
5. Sometimes with erythematous halo.
6. On lips, the ruptured vesicle is covered by a
brownish crust.
7. Degree of pain is quite variable.
1. Antiviral chemotherapeutic
agents such as acyclovir,
vidarabine and idoxuridine.
(Must only be used according
to prescribed indications and
do not represent curative drugs
for this disease.
Buccal mucosa,
soft palate and
tongue
- Most common in
adult life and
affects males and
females.
- Although rare, it
does occur in
children.
Antiviral drugs are now under
intensive clinical testing for
potential effectiveness in
treatment of herpes zoster. The
preliminary results appear very
promising.
1. The varicella-zoster virus
may be spread through the
1. Tongue
2. Buccal Mucosa
Usually occurring
in children and on
1. Patient exhibits fever
2. General malaise
3. Pain with development of clusters of
vesicles over the skin and oral mucosa.
4. Tenderness along the coarse of the
involved sensory nerves, usually unilaterally.
5. Often, trunk is affected.
6. Facial paralysis
7. Pain of the external auditory meatus and
pinna of the ear.
1. The disease begins with fever, headache,
nausea, vomiting, myalgia, sore throat,
- Only palliative treatment is
given, which includes
2. air or by direct contact
with the blisters (lesions)
of someone infected with
chickenpox or shingles.
2. Immunosuppression
such as cytotoxic drug,
radiation, internal
malignancies,
malnutrition, old age, and
alcohol and substance
abuse.
3. Gingival
4. Palate
5. Oropharynx
rare occasions,
nonimmune
adults.
4. Measles (Rubeola;
Morbilli)
1. Direct contact with an
affected person.
2. By droplet of infection,
the portal of entry being
the respiratory tract.
Buccal Mucosa
Primarily affecting
children
5. Mumps (Epidemic
Parotitis)
-Caused by Paramyxovirus
-2-3 weeks incubation
period
-Saliva is the mode of
transmission
Side of the face
under the ears
(the parotid
glands).
Usually a disease
of childhood but
may also affect
adults.
malaise, lung congestion and headache, etc.
2. These are followed by a popular rash first
appearing over the trunk and then rapidly
spreading to face and limbs.
3. After 3 to 4 days, unusual sequences of
macules, vesicles, ulcerations and scabbing of
the skin and oral mucosa are seen.
4. The individual vesicle and ulcerations
appears as “dew drop” on rose petals and is
often surrounded by a zone of erythema at
the periphery.
5. Secondary infection of the vesicles results
in formation of pustules which may leave
small pitting scars upon healing.
6. Small blister-like
7. Not particularly painful
1. Onset of fever
2. Malaise
3. Cough
4. Conjunctivitis
5. Photophobia
6. Lacrimation
7. Eruptive lesion of the skin which begin on
the face, in the hair line and behind the ears,
and spread to the neck, chest, back and
extremities. It would appear as tiny red
papules or macules.
8. Eruptive lesion of the oral mucosa would
appear small, irregularly shaped flecks which
appears bluish, white specks surrounded by a
bright red margin.
9. Palatal and pharyngeal petechiae as well as
generalized inflammation, congestion and
swelling.
10. Focal ulceration of the gingival, palate and
throat may also occur.
1. Headache
2. Chills
3. Moderate fever
4. Vomiting
5. Pain below the ear
6. Firm, somewhat rubbery or elastic swelling
of the salivary glands, frequently elevating
the ear.
antibiotics, antipyretics and
vitamins, etc.
No specific treatment
-Symptomatic supportive
therapy, including bed rest.
-Analgesics may be utilized to
moderate pain.
3. 6. Herpangina
(Aphthous
Pharyngitis; Vesicular
Pharyngitis)
Coxsackie group A viruses
7. Infectious
Mononucleosis
(Glandular Fever)
-Caused by the Epstein B
Virus (EBV)
-Saliva transfer is the
mode of transmission
-EBV associated with cases
of hairy leukoplakia,
Burkitt’s lymphoma &
nasopharyngeal carcinoma
8. Cytomegalic
Inclusion Disease
(Salivary Gland Virus
Disease)
Caused by intrauterine
or early post natal
infection by CMV
(Cytomegalovirus).
Commonly
present in the
posterior hard
and soft palate
(bilateral)
Young chidren,
older children and
adults.
-Occurs chiefly in
children and
young adults (1520 years old)
-No sex or
seasonal
predilection.
Salivary gland
tissue
Majority are
under two years
of age/infants and
few adults.
7. Pain upon mastication
8. “Hamster face” appearance
1. Mild and of short duration.
2. Begins with a sore throat, low grade fever,
headache, sometimes vomiting, prostration
and abdominal pain.
3. Soon will be small ulcers, each showing a
gray base and an inflamed periphery on the
anterior faucial pillars and sometimes on the
hard palates and soft tissues, posterior
pharyngeal wall, buccal mucosa and tongue.
4. Ulcers are not extremely painful, although
dysphagia may occur.
1. Characterized by fever, sore throat,
headache, chills, cough, nausea or vomiting,
lymphadenopathy, pharyngitis and tonsillitis.
2. Prodromal fatigue, anorexia and malaise
usually presents 10-14 days prior to the onset
of fever.
3. Fever usually lasts up to 14 days.
4. Bilateral lymphadenopathy and
oropharyngeal tonsillar enlargements are
common signs.
1. During initial period it produces fever,
malaise, pharyngitis, myalgia and
lymphadenopathy, etc.
2. Retardation of mental and motor
development.
3. Superficial ulcerations or fissures of oral
area; aphthous-like ulcers.
4. Later on there is formation of multiple,
small, fragile vesicles.
5. Soon the fragile vesicles rupture and leave
shallow, pinpoint ulcers.
6. The ulcer often resemble herpetic
infections and each ulcer is surrounded by a
zone of intense erythema (halo)
No treatment is necessary,
since the disease appears to be
self-limiting and presents few
complications.
-No specific treatment.
-NSAIDs and non-aspirin
containing anti-inflammatory
medications may be used for
common symptoms.
-Acyclovir has not been proven
to be clinically effective to this
disease.
- Only palliative treatment is
done.
- Antiherpetic agents: acyclovir,
foscarnet, gancyclovir, cidofovir