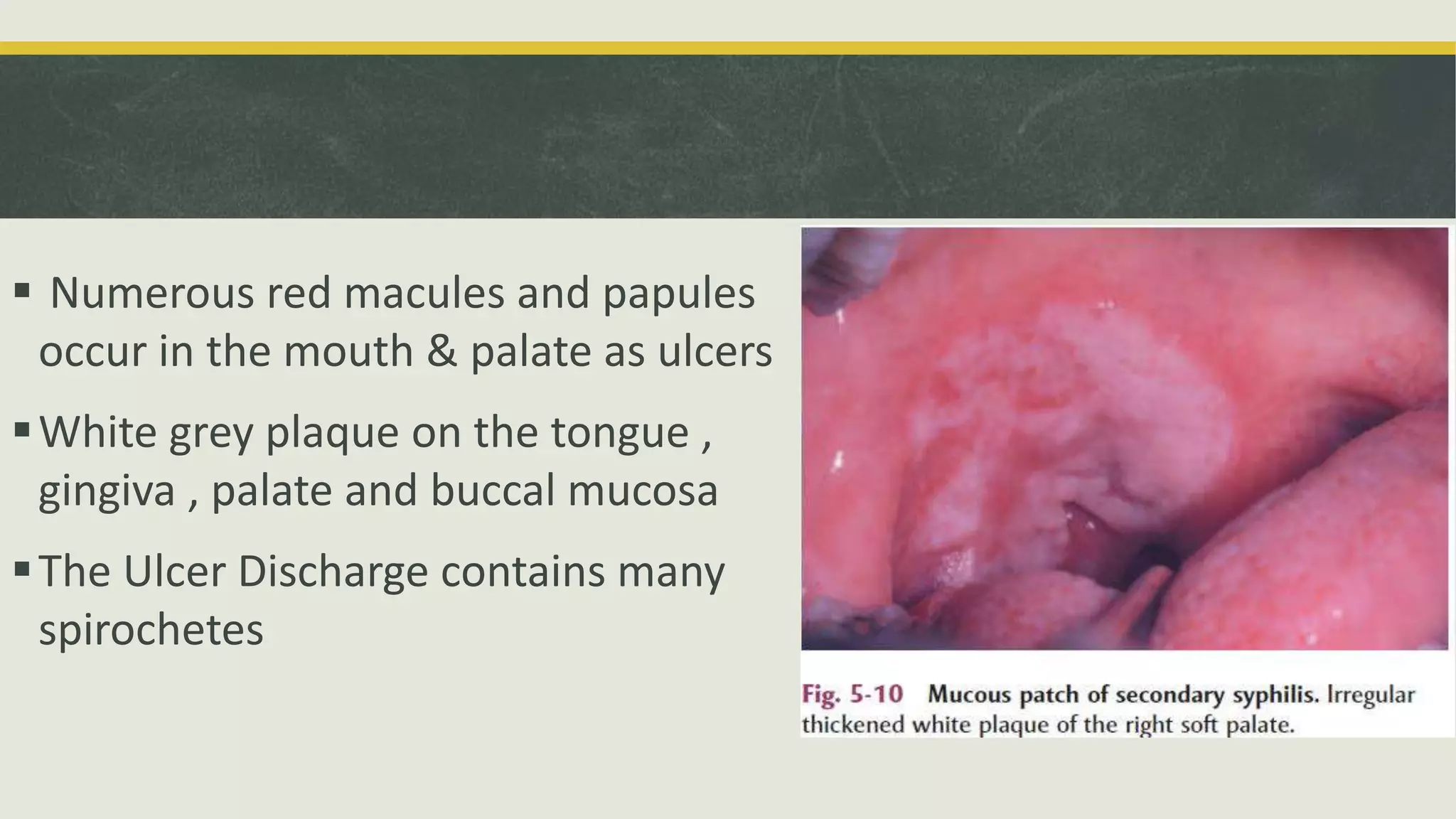
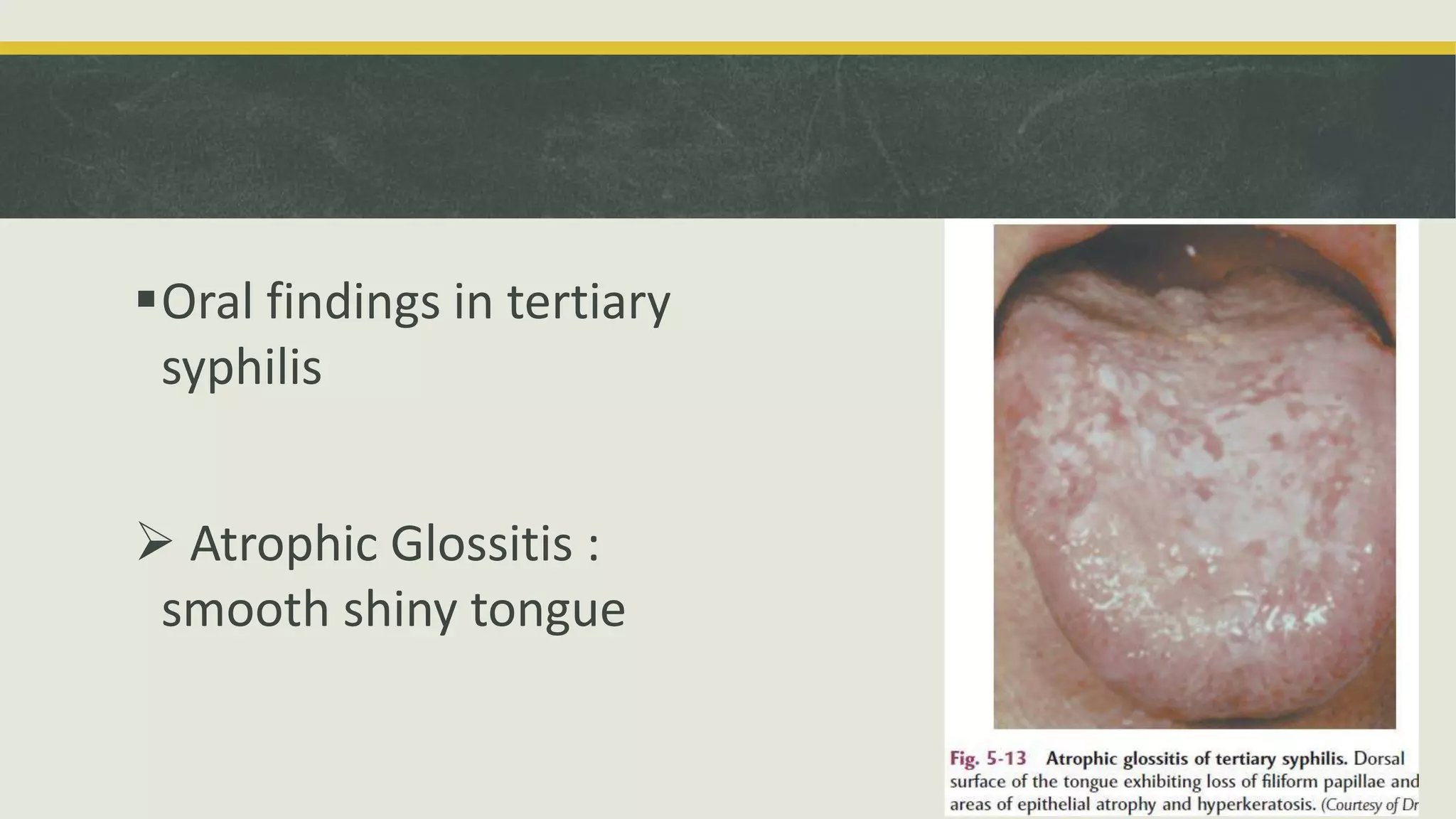
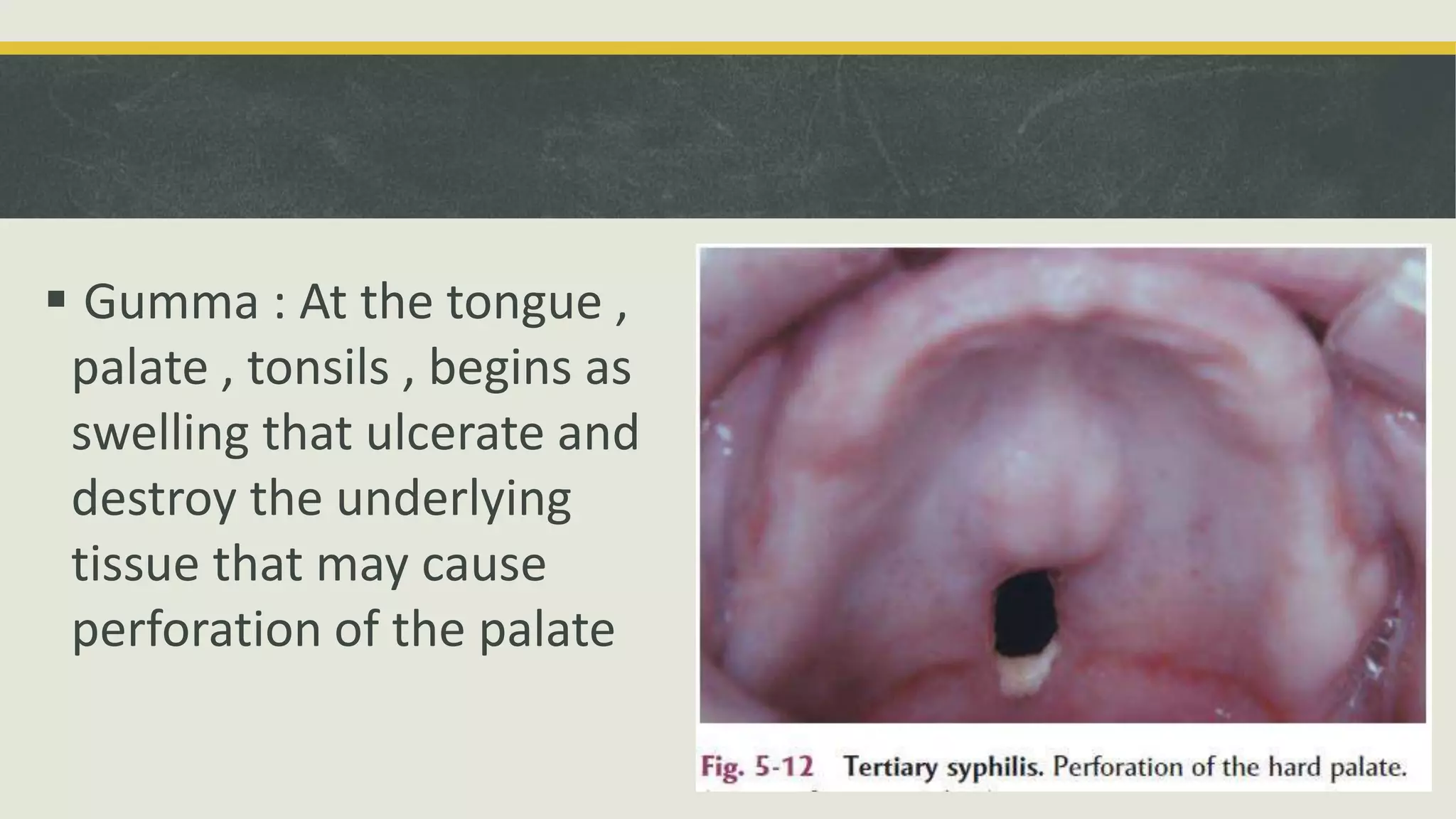
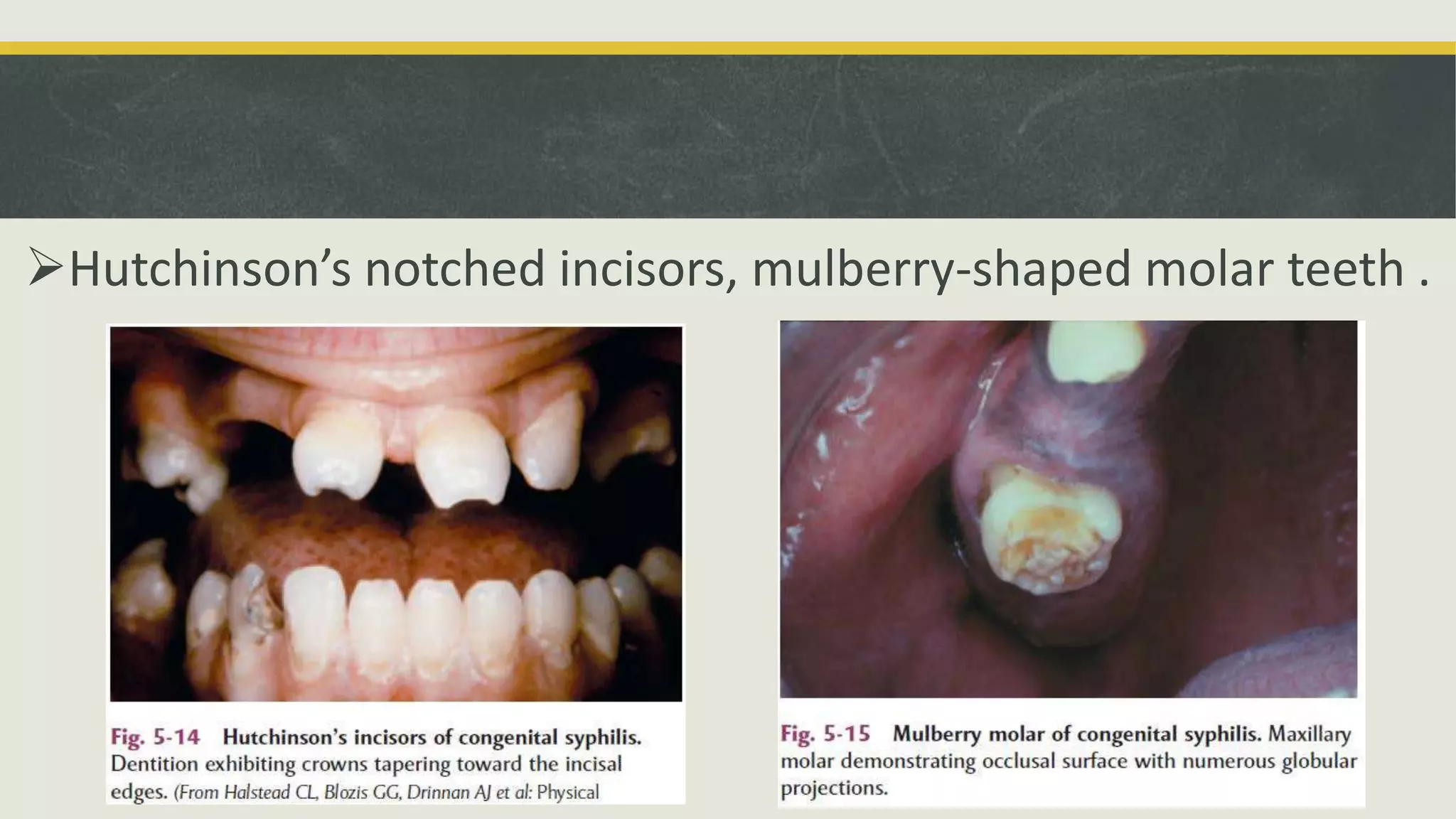
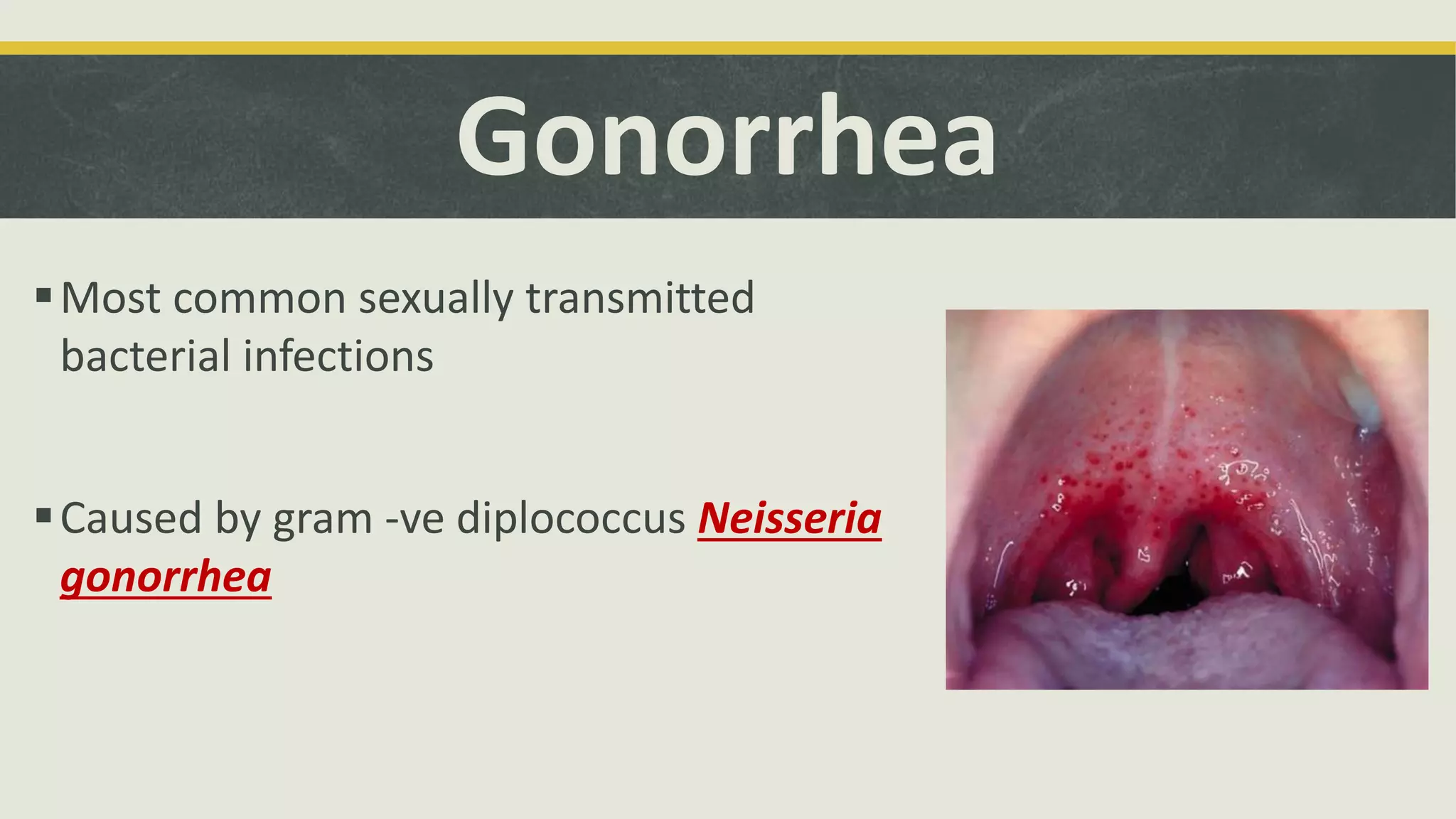
This document provides an overview of several common bacterial infections that can affect the oral cavity. It discusses tuberculosis, which is caused by Mycobacterium tuberculosis and can spread through airborne droplets to the lungs. If the oral cavity is involved, it typically presents as indurated chronic ulcers. Syphilis is caused by Treponema pallidum and has primary, secondary, and tertiary stages marked by chancres, rashes, and potential neurological/cardiovascular effects. Actinomycosis is caused by Actinomyces israelii and usually appears in the jaw after trauma or infection, causing hard swellings that may drain through the gums. Gonorrhea, caused by Ne