The AssignmentExamine Case Study A Young Caucasian Girl W.docxrtodd17
The Assignment
Examine
Case Study: A Young Caucasian Girl With ADHD
You will be asked to make three decisions concerning the medication to prescribe to this client. Be sure to consider factors that might impact the client’s pharmacokinetic and pharmacodynamic processes.
At each decision point stop to complete the following:
At each decision point stop to complete the following:
Decision #1
Which decision did you select?
Why did you select this decision? Support your response with evidence and references to the Learning Resources.
What were you hoping to achieve by making this decision? Support your response with evidence and references to the Learning Resources.
Explain any difference between what you expected to achieve with Decision #1 and the results of the decision. Why were they different?
Decision #2
Why did you select this decision? Support your response with evidence and references to the Learning Resources.
What were you hoping to achieve by making this decision? Support your response with evidence and references to the Learning Resources.
Explain any difference between what you expected to achieve with Decision #2 and the results of the decision. Why were they different?
Decision #3
Why did you select this decision? Support your response with evidence and references to the Learning Resources.
What were you hoping to achieve by making this decision? Support your response with evidence and references to the Learning Resources.
Explain any difference between what you expected to achieve with Decision #3 and the results of the decision. Why were they different?
case Study and the decisions
BACKGROUND
Katie is an 8 year old Caucasian female who is brought to your office today by her mother & father. They report that they were referred to you by their primary care provider after seeking her advice because Katie’s teacher suggested that she may have ADHD. Katie’s parents reported that their PCP felt that she should be evaluated by psychiatry to determine whether or not she has this condition.
The parents give the PMHNP a copy of a form titled
“Conner’s Teacher Rating Scale-Revised”.
This scale was filled out by Katie’s teacher and sent home to the parents so that they could share it with their family primary care provider. According to the scoring provided by her teacher, Katie is inattentive, easily distracted, forgets things she already learned, is poor in spelling, reading, and arithmetic. Her attention span is short, and she is noted to only pay attention to things she is interested in. The teacher opined that she lacks interest in school work and is easily distracted. Katie is also noted to start things but never finish them, and seldom follows through on instructions and fails to finish her school work.
Katie’s parents actively deny that Katie has ADHD. “She would be running around like a wild pers.
What is Attention-Deficit/Hyperactivity Disorder?
Inattentive, hyperactive & impulsive to excessive degree compared with their peers.
For more info, download the presentation.
Babatunde Idowu Ogundipe M.D. M.P.H.
Comprehensive Clinical Services P.C.
October 7 2011
Global Medical Cures™ | Attention Deficit Hyperactivity Disorder (ADHD) Global Medical Cures™
Global Medical Cures™ | Attention Deficit Hyperactivity Disorder (ADHD)
~10% of kids in the US are prescribed ADHD drugs and this trend is also growing worldwide. Find out more about ADHD in this booklet.
DISCLAIMER-
Global Medical Cures™ does not offer any medical advice, diagnosis, treatment or recommendations. Only your healthcare provider/physician can offer you information and recommendations for you to decide about your healthcare choices.
This is a fascinating and informative introduction to the causes, consequences, diagnosis and treatment of ADHD. It is appropriate for parents, teachers, undergraduate and graduate students.
The AssignmentExamine Case Study A Young Caucasian Girl.docxrtodd17
The Assignment
Examine
Case Study: A Young Caucasian Girl With ADHD
You will be asked to make three decisions concerning the medication to prescribe to this client. Be sure to consider factors that might impact the client’s pharmacokinetic and pharmacodynamic processes.
At each decision point stop to complete the following:
·
Decision #1
o Which decision did you select?
o Why did you select this decision? Support your response with evidence and references to the Learning Resources.
o What were you hoping to achieve by making this decision? Support your response with evidence and references to the Learning Resources.
o Explain any difference between what you expected to achieve with
Decision #1 and the results of the decision. Why were they different?
·
Decision #2
o Why did you select this decision? Support your response with evidence and references to the Learning Resources.
o What were you hoping to achieve by making this decision? Support your response with evidence and references to the Learning Resources.
o Explain any difference between what you expected to achieve with Decision #2 and the results of the decision. Why were they different?
·
Decision #3
o Why did you select this decision? Support your response with evidence and references to the Learning Resources.
o What were you hoping to achieve by making this decision? Support your response with evidence and references to the Learning Resources.
o Explain any difference between what you expected to achieve with
o Decision #3 and the results of the decision. Why were they different?
Also include how ethical considerations might impact your treatment plan and communication with clients.
Note: Support your rationale with a minimum of three academic resources no more than five years old in APA Format
Attention Deficit Hyperactivity Disorder
A Young Girl With ADHD
BACKGROUND
Katie is an 8 year old Caucasian female who is brought to your office today by her mother & father. They report that they were referred to you by their primary care provider after seeking her advice because Katie’s teacher suggested that she may have ADHD. Katie’s parents reported that their PCP felt that she should be evaluated by psychiatry to determine whether or not she has this condition.
The parents give the PMHNP a copy of a form titled
“Conner’s Teacher Rating Scale-Revised”.
This scale was filled out by Katie’s teacher and sent home to the parents so that they could share it with their family primary care provider. According to the scoring provided by her teacher, Katie is inattentive, easily distracted, forgets things she already learned, is poor in spelling, reading, and arithmetic. Her attention span is short, and she is noted to only pay attention to things she is interested in. The teacher opined that she lacks interest in school work and is easily distracted. Katie is also noted to start things but never finish them, and seldom follows through on in.
Attention Deficit disorder with its etiology, types and pathophysiology clinical features, Diagnosis, Assessment, differential Diagnosis and treatment , Medical Treatment and prognosis
Plan of WorkGloria is employed at Jones University, through .docxJUST36
Plan of Work
Gloria is employed at Jones University, through Higher Learning Systems in Connecticut as a data entry specialist. She originally worked for Higher Learning Systems in Canada; but, she transferred with her husband to the United States through his military career. Gloria has been employed with Higher Learning Systems for 6 years. She worked 5 years in Canada and has been in Connecticut for one year. She was on medical leave for 6 months due to her pregnancy with her first child. She had complications and was absent from work for 3 months before the birth of her child.
There are 12 data entry specialists at Jones University in Connecticut. When Gloria took leave unexpectedly, the other 11 specialists had to split up her work duties. After the birth of Gloria’s child, her co-workers were upset that she decided to take off 12 weeks after the birth, despite the fact she was out 12 weeks before the delivery. When Gloria returned to work, she took frequent breaks, more than the policy allowed, to pump and securely store breast milk for her infant. Since these breaks interfered with her workload, the 11 employees were required to carry a percent of Gloria’s workload until she decided to stop pumping and storing breast milk at work. Employees were extremely frustrated at Gloria and felt as though the university was giving her special treatment.
Gloria felt the frustration immediately when returning to work, despite the fact that the university had indicated that it supported mothers on parental leave and mothers who needed extra time to pump breast milk after maternity leave. She felt disrespected by her co-workers due to her cultural beliefs about the importance of breast feeding. The discomfort she felt affected her work, and she began to fall further behind in her daily responsibilities. Soon, she dreaded going to work, cried often, and felt unappreciated by her supervisor. She also felt her supervisor did not approve of her decision to take 12 weeks off after her infant was born and she didn’t approve of her frequent breaks. Gloria often overheard other employees making jokes about her. Gloria has worked for the company for 6 years and does not want to quit. She decides to visit Human Resources for assistance. Human Resources works with Gloria and her supervisor to create a plan of work to assist with the areas of concern.
For this assignment, there are three main parts: first summarize the scenario, second outline Human Resources response to Gloria, and third prepare a plan of work for Gloria and her supervisor. The plan of work is prepared by Human Resources, so it should include goals for Gloria, the supervisor, and/or the department. Include a timeline with the goals. Ensure the goals are measurable and attainable.
Length: 6 pages, not including title and reference pages " 1 title, 6 body, 1 reference "
References: Include a minimum of five scholarly resources.
Your paper should demonstrate thoughtf.
Planning, Implementation, and Evaluation Evaluate the importa.docxJUST36
Planning, Implementation, and Evaluation"
Evaluate the importance of each major step in policy analysis as it relates to political choice. Next, debate if one would consider any of these steps more important than another. Provide a rationale to support your answer.
From the e-Activity, Next, suggest one (1) method that a policy analyst could use in order to implement the strategic plan overall. Provide a rationale to support yo
.
More Related Content
Similar to PATIENT FILE151PATIENT FILEThe Case The scatter-b.docx
The AssignmentExamine Case Study A Young Caucasian Girl W.docxrtodd17
The Assignment
Examine
Case Study: A Young Caucasian Girl With ADHD
You will be asked to make three decisions concerning the medication to prescribe to this client. Be sure to consider factors that might impact the client’s pharmacokinetic and pharmacodynamic processes.
At each decision point stop to complete the following:
At each decision point stop to complete the following:
Decision #1
Which decision did you select?
Why did you select this decision? Support your response with evidence and references to the Learning Resources.
What were you hoping to achieve by making this decision? Support your response with evidence and references to the Learning Resources.
Explain any difference between what you expected to achieve with Decision #1 and the results of the decision. Why were they different?
Decision #2
Why did you select this decision? Support your response with evidence and references to the Learning Resources.
What were you hoping to achieve by making this decision? Support your response with evidence and references to the Learning Resources.
Explain any difference between what you expected to achieve with Decision #2 and the results of the decision. Why were they different?
Decision #3
Why did you select this decision? Support your response with evidence and references to the Learning Resources.
What were you hoping to achieve by making this decision? Support your response with evidence and references to the Learning Resources.
Explain any difference between what you expected to achieve with Decision #3 and the results of the decision. Why were they different?
case Study and the decisions
BACKGROUND
Katie is an 8 year old Caucasian female who is brought to your office today by her mother & father. They report that they were referred to you by their primary care provider after seeking her advice because Katie’s teacher suggested that she may have ADHD. Katie’s parents reported that their PCP felt that she should be evaluated by psychiatry to determine whether or not she has this condition.
The parents give the PMHNP a copy of a form titled
“Conner’s Teacher Rating Scale-Revised”.
This scale was filled out by Katie’s teacher and sent home to the parents so that they could share it with their family primary care provider. According to the scoring provided by her teacher, Katie is inattentive, easily distracted, forgets things she already learned, is poor in spelling, reading, and arithmetic. Her attention span is short, and she is noted to only pay attention to things she is interested in. The teacher opined that she lacks interest in school work and is easily distracted. Katie is also noted to start things but never finish them, and seldom follows through on instructions and fails to finish her school work.
Katie’s parents actively deny that Katie has ADHD. “She would be running around like a wild pers.
What is Attention-Deficit/Hyperactivity Disorder?
Inattentive, hyperactive & impulsive to excessive degree compared with their peers.
For more info, download the presentation.
Babatunde Idowu Ogundipe M.D. M.P.H.
Comprehensive Clinical Services P.C.
October 7 2011
Global Medical Cures™ | Attention Deficit Hyperactivity Disorder (ADHD) Global Medical Cures™
Global Medical Cures™ | Attention Deficit Hyperactivity Disorder (ADHD)
~10% of kids in the US are prescribed ADHD drugs and this trend is also growing worldwide. Find out more about ADHD in this booklet.
DISCLAIMER-
Global Medical Cures™ does not offer any medical advice, diagnosis, treatment or recommendations. Only your healthcare provider/physician can offer you information and recommendations for you to decide about your healthcare choices.
This is a fascinating and informative introduction to the causes, consequences, diagnosis and treatment of ADHD. It is appropriate for parents, teachers, undergraduate and graduate students.
The AssignmentExamine Case Study A Young Caucasian Girl.docxrtodd17
The Assignment
Examine
Case Study: A Young Caucasian Girl With ADHD
You will be asked to make three decisions concerning the medication to prescribe to this client. Be sure to consider factors that might impact the client’s pharmacokinetic and pharmacodynamic processes.
At each decision point stop to complete the following:
·
Decision #1
o Which decision did you select?
o Why did you select this decision? Support your response with evidence and references to the Learning Resources.
o What were you hoping to achieve by making this decision? Support your response with evidence and references to the Learning Resources.
o Explain any difference between what you expected to achieve with
Decision #1 and the results of the decision. Why were they different?
·
Decision #2
o Why did you select this decision? Support your response with evidence and references to the Learning Resources.
o What were you hoping to achieve by making this decision? Support your response with evidence and references to the Learning Resources.
o Explain any difference between what you expected to achieve with Decision #2 and the results of the decision. Why were they different?
·
Decision #3
o Why did you select this decision? Support your response with evidence and references to the Learning Resources.
o What were you hoping to achieve by making this decision? Support your response with evidence and references to the Learning Resources.
o Explain any difference between what you expected to achieve with
o Decision #3 and the results of the decision. Why were they different?
Also include how ethical considerations might impact your treatment plan and communication with clients.
Note: Support your rationale with a minimum of three academic resources no more than five years old in APA Format
Attention Deficit Hyperactivity Disorder
A Young Girl With ADHD
BACKGROUND
Katie is an 8 year old Caucasian female who is brought to your office today by her mother & father. They report that they were referred to you by their primary care provider after seeking her advice because Katie’s teacher suggested that she may have ADHD. Katie’s parents reported that their PCP felt that she should be evaluated by psychiatry to determine whether or not she has this condition.
The parents give the PMHNP a copy of a form titled
“Conner’s Teacher Rating Scale-Revised”.
This scale was filled out by Katie’s teacher and sent home to the parents so that they could share it with their family primary care provider. According to the scoring provided by her teacher, Katie is inattentive, easily distracted, forgets things she already learned, is poor in spelling, reading, and arithmetic. Her attention span is short, and she is noted to only pay attention to things she is interested in. The teacher opined that she lacks interest in school work and is easily distracted. Katie is also noted to start things but never finish them, and seldom follows through on in.
Attention Deficit disorder with its etiology, types and pathophysiology clinical features, Diagnosis, Assessment, differential Diagnosis and treatment , Medical Treatment and prognosis
Plan of WorkGloria is employed at Jones University, through .docxJUST36
Plan of Work
Gloria is employed at Jones University, through Higher Learning Systems in Connecticut as a data entry specialist. She originally worked for Higher Learning Systems in Canada; but, she transferred with her husband to the United States through his military career. Gloria has been employed with Higher Learning Systems for 6 years. She worked 5 years in Canada and has been in Connecticut for one year. She was on medical leave for 6 months due to her pregnancy with her first child. She had complications and was absent from work for 3 months before the birth of her child.
There are 12 data entry specialists at Jones University in Connecticut. When Gloria took leave unexpectedly, the other 11 specialists had to split up her work duties. After the birth of Gloria’s child, her co-workers were upset that she decided to take off 12 weeks after the birth, despite the fact she was out 12 weeks before the delivery. When Gloria returned to work, she took frequent breaks, more than the policy allowed, to pump and securely store breast milk for her infant. Since these breaks interfered with her workload, the 11 employees were required to carry a percent of Gloria’s workload until she decided to stop pumping and storing breast milk at work. Employees were extremely frustrated at Gloria and felt as though the university was giving her special treatment.
Gloria felt the frustration immediately when returning to work, despite the fact that the university had indicated that it supported mothers on parental leave and mothers who needed extra time to pump breast milk after maternity leave. She felt disrespected by her co-workers due to her cultural beliefs about the importance of breast feeding. The discomfort she felt affected her work, and she began to fall further behind in her daily responsibilities. Soon, she dreaded going to work, cried often, and felt unappreciated by her supervisor. She also felt her supervisor did not approve of her decision to take 12 weeks off after her infant was born and she didn’t approve of her frequent breaks. Gloria often overheard other employees making jokes about her. Gloria has worked for the company for 6 years and does not want to quit. She decides to visit Human Resources for assistance. Human Resources works with Gloria and her supervisor to create a plan of work to assist with the areas of concern.
For this assignment, there are three main parts: first summarize the scenario, second outline Human Resources response to Gloria, and third prepare a plan of work for Gloria and her supervisor. The plan of work is prepared by Human Resources, so it should include goals for Gloria, the supervisor, and/or the department. Include a timeline with the goals. Ensure the goals are measurable and attainable.
Length: 6 pages, not including title and reference pages " 1 title, 6 body, 1 reference "
References: Include a minimum of five scholarly resources.
Your paper should demonstrate thoughtf.
Planning, Implementation, and Evaluation Evaluate the importa.docxJUST36
Planning, Implementation, and Evaluation"
Evaluate the importance of each major step in policy analysis as it relates to political choice. Next, debate if one would consider any of these steps more important than another. Provide a rationale to support your answer.
From the e-Activity, Next, suggest one (1) method that a policy analyst could use in order to implement the strategic plan overall. Provide a rationale to support yo
.
Planet of the Apes (1974) (Race relations and slavery—turnabout is .docxJUST36
Planet of the Apes (1974): (Race relations and slavery—turnabout is fair play?)
Romeo and Juliet, Shakespeare 1996 (film)
Les Miserables, Victor Hugo 1998 (film)
The Crucible, Arthur Miller 1996 (film)
Death of a Salesman, Arthur Miller 2001 (film)
The Great Gatsby T.S. Elliot 2000 (film)
The Count of Monte Cristo, Alexander Dumas 2002 (film)
Saving Private Ryan: (Saving the last family to survive WWII combat)
Avatar: (The displacement of native populations)
Jurassic Park (1993): (Science and Ethics)
A Few Good Men: (Following illegal orders in the military service)
Pick 5, each should have a separate paper.
Write a short written report on the
ethical issues
expressed in 5 of these films.
Limit the length to one and a half pages, double spaced. Try to pick out the most important ethical issues and explain how they are handled in the film. (Do not give simple plot conditions and character types—get to the heart of the ethical issues and how they are treated, that is, talk about the morality play that is being presented.)
.
Planning effective English language arts lessons many times incl.docxJUST36
Planning effective English language arts lessons many times includes focusing on multiple literacy skills, aligned to state or national standards, while incorporating interesting, student-centered materials. When focusing on reading, it is essential to model metacognitive strategies, before, during, and after reading, including relevant vocabulary. A book walk is a powerful pre-reading strategy that can be used at all elementary grade levels. This strategy exposes students to a new piece of literary or informative text, while predicting text content and exploring vocabulary.
Throughout this course you will be creating a literature unit based on one piece of grade-appropriate literature (fiction or non-fiction) that includes all areas of reading development. Select a piece of literature suitable for the students in the “Class Profile.”
For this assignment, use the “COE Lesson Plan Template” to create a lesson plan that incorporates a book walk,
Incorporate the following into your lesson plan:
Objectives aligned to state or national grade-appropriate vocabulary and reading standards
Content-specific vocabulary development
Technology or multimedia that supports developmentally appropriate, engaging instruction
Pre-reading strategies and activities
During reading strategies and activities
Post-reading activities and strategies
Assessment aligned to learning objectives, that is engaging for student and provides meaningful feedback
Differentiation to meet particular learning differences or needs
In addition, rationalize your instructional choices in a 250-500 word reflection, including how you will apply your findings to personal professional practices related to instruction and differentiation in the English language arts classroom
.
PKI Submission RequirementsFormat Microsoft WordFon.docxJUST36
PKI
Submission Requirements
Format: Microsoft Word
Font: Arial, 12-Point, Double-Space
Citation Style: APA
Length: 1–2 pages
Self-Assessment Checklist
Use the following checklist to support your work on the assignment:
I have identified specific data types related to the specific compliance regulatory requirements.
I have indicated a solution for sharing data beyond the borders of the organization.
I have appropriately selected and developed a PKI solution for content control.
I have followed the submission requirements.
.
PLAGIARISM SCAN REPORT
Date 2020-04-12
Words 161
Characters 991
Content Checked For Plagiarism
Stereolithography (SLA) is one method of many used for 3D printing. There are roughly 30 different processes for additive manufacturing
(commonly called 3D printing) used for different materials from plastics, metals, ceramics, clay, concrete, chocolate, pancake batter and other
foodstuffs, paper, and sand (silica) to living tissue and cells. SLA was one of the earlier 3D methods first developed around 1984. Commercial
SLA printers originally cost hundreds of thousands of dollars, but can now be purchased for a few hundred or a few thousand dollars or even
built at home for less [1]. In the SLA process a liquid material called a photo-polymer is exposed to light from a laser, from a digital projector,
or from another focused optical source. The radiation causes the material to solidify (or cure) where the light hits it. When the full object has
been “drawn”, it is removed from the tank holding the liquid polymer. And there you have your “heart’s desire” in your hand.
Matched Source
Similarity 89%
Title: What is stereolithography used for? - Quora | How it works: SLA
stereolithography (sla) is one method of many used for 3d printing. there are roughly 30 different processes for additive manufacturing
(commonly called 3d printing) used for different materials from plastics, metals, ceramics, clay, concrete, chocolate, pancake batter and
other...
https://www.quora.com/What-is-stereolithography-used-for
Similarity 12%
Title: 1 John commentary - Scripture Verse By Verse
... and a coke and unwraps it for you and puts it in your hand don't blame him if ... A hatred for sin; a desire to please God and confession
when we fail are ... If you hate someone you have murdered them in your heart as far as God is concerned. ... fact that Jesus is God and
savior and there you have your three witnesses. 9.
https://www.thebibleversebyverse.com/1-john-commentary.html
100%
Plagiarised
0%
Unique
https://www.quora.com/What-is-stereolithography-used-for
https://www.quora.com/What-is-stereolithography-used-for
https://www.quora.com/What-is-stereolithography-used-for
https://www.thebibleversebyverse.com/1-john-commentary.html
https://www.thebibleversebyverse.com/1-john-commentary.html
https://www.thebibleversebyverse.com/1-john-commentary.html
Motivation and Emotion:
Driving Consumer Behavior
Chapter 5
Motivation
Types:
Homeostasis
Maintain yourself in a current acceptable state
Self improvement
Desire to change yourself to a more ideal state
Exercise
Think of something of something you have purchased because you wanted something thing to remain the same (homeostasis)
Think of something you have purchased because you wanted something to change (self improvement)
Other ways to look at motivations
Utilitarian
Desire to acquire products that can be used to accomplish things
Hedonic
Desire to experience something personally grat.
Plato’s Apology The Trial of SocratesSocrates in the trial .docxJUST36
Plato’s Apology: The Trial of Socrates
Socrates in the trial – speaking plainly, daily converse. He is a speaker of the truth, not an accomplished speaker.
Socrates’ accusers:
1. Meletus
2. Anytus
3. Lycon
Why does he fear the early accusers more than the recent ones?
They’re anonymous, they are shadows, rumours brainwashed children of that period are now jurors who will decide his fate, they’re nameless, cannot bring evidence forward. They corrupted mind of jurors.
• Children grew hearing that Socrates is a trouble maker, their minds have been infected since they could not ask any acquisitions.
• They accepted this truth and now deciding his fate with prejudice against him they developed when they were kids. He cannot do anything about the prejudices.
• You cannot argue with phantom, ghosts, cannot address them in a straightforward manner.
He fears them the most, they are formidable, because he exposes them for having a reputation of wisdom while they know little, he broke their façade, exposed their flaws hence they may go to any lengths to take vengeance. He exposed people’s ignorance = made himself a lot of enemies.
They accused him of being a Sophist, bad reputation during his time, teaching people weak arguments, weak ideas for money. Socrates was not a sophist. This is what the early accusers made them believe. Sophists were doubtful of God. The 500 jurors never got to hear Socrates speak, they’re just brainwashed.
Socrates’ Attitude during the trial:
• Kind of saying take it easy on me, old man in court for the first time. “I’m a stranger to the court room, treat me kindly”
• Tries to appeal to their humanness, the jurors.
The story of the oracle (Delphi) – temple of Apollo
Oracle is like a messenger, knowledge she has is provided by the gods. The wisdom was unnatural. One of Socrates followers asked the Oracle who is the wisest, is there wiser than Socrates? The God answered no. Socrates was in disbelief, he knew he was unwise.
So he questioned people and learns that people have a reputation to be wise, yet they know nothing and pretend to know. They continue this charade of wisdom because they’re reputation is built on it. He questioned craftsmen, politicians, poets
In the sight of god: wisdom means nothing, like Socrates, we should not pretend more than we are. True wisdom = not knowing.
“Socrates, the gadfly of Athen”
He was proud of the fact that he was like a fly, an irritant. Gadfly = horse fly. He believes this type of insect is necessary. He compares himself to the gadfly and the horse that the gadfly bites is Athens. Gods put Socrates as a gadfly to wake Athens up. Rousing, reproaching, scolding is a good thing. People do not want to be questioned, be shammed, have their knowledge punctured. He compares this to as though the person who wakes you up, you’d naturally be mad.
Philosophy is dangerous but necessary. Living well is more important than living. Die well is better than to live.
W3 C2 – Plato’s Apology
A.
Pine tree tops” by Gary SnyderIn the blue night frost haze,.docxJUST36
“Pine tree tops” by Gary Snyder
In the blue night
frost haze, the sky glows
with the moon
pine tree tops
bend snow-blue, fade
into sky, frost, starlight.
The creak of boots. Rabbit tracks, deer tracks,
what do we know.
writing thesis statement for this poem,
for example: Snyder builds his poem on nouns to give power to the “thing” in his scene.
.
Platform as a Service (PaaS) and Infrastructure as a Service (I.docxJUST36
"Platform as a Service (PaaS) and Infrastructure as a Service (IaaS)" Please respond to the following:
Examine how IaaS and PaaS trends in cloud computing will impact enterprise security policies in the short and long term. Support your findings with an example of each service in the cloud computing stack.
Differentiate between physical, dedicated virtual, and shared virtual servers
.
plan for your client Eliza. Since the initial treatment plan, severa.docxJUST36
plan for your client Eliza. Since the initial treatment plan, several changes have taken place within Eliza’s case. Since the mandatory assessment two weeks ago, you have discovered that Eliza is again on your client listing for the day due to a mandatory evaluation, with the incident report indicating that campus public safety, due to a tip from a concerned resident, found the client passed out and alone in her dorm, smelling of alcohol.
Part 1: Review the initial Treatment Plan submitted in Topic 5.
Reassess your treatment plan diagnoses, goals, and objectives based on the new information provided.
.
Plan a geographic inquiry to investigate the question. In the pl.docxJUST36
Plan a geographic inquiry to investigate the question. In the plan students will explain how they will complete the following aspects of the investigation
a. Investigating cultural perceptions of land and land use
b. Collecting primary and secondary data c. Analysing data
d. Mapping the study area, data and results
e. Communicate results
.
PLAGIARISMWhat is it Whose Responsibility is It Wha.docxJUST36
PLAGIARISM:
What is it?
Whose Responsibility is It?
What Are the Consequences?
A Brief Guide
Department of Management
CBPA, CSUSB
This presentation meets ADA compliance criteria for posting to CSUSB websites
Plagiarism is a Serious Problem
in Academia
“A study of almost 4,500 students at 25 schools,
suggests cheating is . . . a significant problem in
high school - 74% of the respondents admitted to
one or more instances of serious test cheating
and 72% admitted to serious cheating on written
assignments. Over half of the students admitted
they have engaged in some level of plagiarism
on written assignments using the Internet.”
Based on the research of Donald L. McCabe, Rutgers University.
Source: “CIA Research.” Center for Academic Integrity, Duke University, 2003
<http://academicintegrity.org/cai_research.asp>.
http://academicintegrity.org/cai_research.asp
The Student’s Responsibility
• A student should be clear that work submitted for
a grade in the class must be original work.
• It is the responsibility of the student to become
fully acquainted with what constitutes
plagiarism.
• A student can check his/her writing in
Turnitin.com to see whether material shows us
that he/she may have advertently or unknowingly
used that is not their own. (However, it is up to
the instructor to determine plagiarized material )
• The student must correct the error with an
appropriate citation.
Instructor’s Responsibility
The Instructor is responsible for drawing a
conclusion regarding whether the amount of
improperly attributed or unattributed material
is so significant that intent may be presumed.
Excuses Won’t Work
The
teacher
treated me
unfairly,
so I feel
O.K. doing
it!
My job takes up too
much time, plus I am a
caregiver to my younger siblings
My classmates
Are going to
Berkeley
& I want to go
Too!
Students sometimes claim
“Accidental” or “Unintentional Plagiarism”--
What is This?
• Not knowing how/when to cite sources
• Plagiarism vs. paraphrasing
• Careless paraphrasing
• Uncertainty over what is a fact or common
knowledge
• Not knowing what constitutes research
• Quoting excessively
• Different view of plagiarism based on cultural
background
• NOTE: It is the responsibility of the student to become
fully acquainted with what constitutes plagiarism
Disciplinary Consequences
• See pages 53-54, “Plagiarism and Cheating”
CSUSB University Catalog/Bulletin for
violations and consequences.
Pay Attention to Avoiding Even the
Appearance of Plagiarism
WHAT IS PLAGIARISM?: It is use of the following
without giving credit to:
another person’s idea, opinion, or theory;
any facts, statistics, graphs, drawings, and audio
extractions from another’s work;
Any information that is not in the realm of common
knowledge;
quotations of another person’s actual spoken or
written words;
paraphrasing another person’s spoken or written words
without givin.
PKI and Encryption at WorkLearning Objectives and Outcomes· De.docxJUST36
PKI and Encryption at Work
Learning Objectives and Outcomes
· Develop a plan to deploy public key infrastructure (PKI) and encryption solutions to protect data and information.
Assignment Requirements
In this assignment, you play the role of chief information technology (IT) security officer for the Quality Medical Company (QMC). QMC is a publicly traded company operating in the pharmaceutical industry.
QMC is expanding its arena of work through an increase in the number of clients and products. The senior management of the company is highly concerned about complying with the multitude of legislative and regulatory laws and issues in place. The company has an internal compliance and risk management team to take care of all the compliance-related issues. The company needs to make important decisions about the bulk of resources they will need to meet the voluminous compliance requirements arising from the multidimensional challenge of expansion.
QMC will be required to conform to the following compliance issues:
· Public-company regulations, such as the Sarbanes-Oxley (SOX) Act
· Regulations affecting financial companies, companies that make loans and charge interest, such as the U.S. Securities and Exchange Commission (SEC) rules and Gramm-Leach-Bliley Act (GLBA)
· Regulations affecting healthcare privacy information, such as Health Insurance Portability and Accountability Act (HIPAA)
· Intellectual Property Law that is important for information asset protection particularly for organizations in the pharmaceutical and technology industry
· Regulations affecting the privacy of information, including personal identification information, such as personally identifiable information (PII) regularly collected from employees, customers, and end users
· Corporate governance policies including disclosures to the board of directors and the auditors and the policies related to human resources, governance, harassment, code of conduct, and ethics
Compliance with regulatory requirements implies encrypting sensitive data at rest (DAR) and allowing access to role-holders in the enterprise who require the access. It also implies that sensitive data in motion (DIM) or data that is being communicated via e-mail, instant message (IM), or even Web e-mail must be suitably protected and sent only to the individuals who have a right to view it. The company is conscious about the loss they may face in terms of penalty and brand damage if they fail to abide by the compliance laws, especially in the online information transfer phase. Therefore, as a dedicated employee, your task is to develop a content monitoring strategy using PKI as a potential solution. You will need to determine a process or method to identify multiple data types, processes, and organizational policies. Incorporate them into a plan, and select a PKI solution that will effectively address the content management needs of your company.
You need to present your PKI solution in the form of a profes.
Pine Valley Furniture wants to use Internet systems to provide value.docxJUST36
Pine Valley Furniture wants to use Internet systems to provide value to its customers and staff. There are many software technologies available to internet systems development teams, including SOAP, HTML, JSON, XML, CSS, ASP.NET, Objective C, php, JAVA™, Python, Ruby, AJAX, Swift™, AngularJS, Bootstrap, jQuery, R, and many more.
Create
a 3- to 4-page comparison table or tabbed spreadsheet and supporting narrative that addresses the items listed below. Analyze and compare at least three internet systems development software technologies for use at PVF.
Analyze
how the selected internet systems development software technologies support PVF’s core business processes.
Compare
the selected technologies and then the reasons why, as an internet systems developer, you might choose one technology over another technology for PVF.
Explain
how these technologies can bring value to PVF.
Incorporate
additional research to support your comparison.
Cite
any references according to APA guidelines.
.
Pick the form of cultural expression most important to you. It could.docxJUST36
Pick the form of cultural expression most important to you. It could be music, theater, dance, visual arts—whatever excites and/or inspires you most. Describe:
Its most significant characteristics (e.g., visual, audio, etc.)
Your favorite artists in this art, and why.
The one example of this art that inspires you most.
500 words
.
Pick two diseases from each of the following systems HEENT .docxJUST36
Pick two diseases from each of the following systems:
HEENT :
1.
Glaucoma 2. Conjunctivitis
Pulmonary:
1.
Asthma 2. Pneumonia
Hematology:
1.
Anemia. 2. Sickle Cell Anemia
Neurology:
1.
Epilepsy 2. Migraines
Gastroenterology:
1.
Gastroesophageal reflux 2. irritable bowel disease
Cardiovascular:
1.
Coronary artery disease 2. Atrial Fibrillation
Orthopedics:
1.
Carpal Tunnel Syndrome 2. Arthritis
Endocrinology:
1.
Hypothyroidism 2. Hyperthyroidism
Dermatology:
1.
Eczema 2.Rosacea
Urology and STD’s:
1.
Hematuria 2. prostatitis
Pregnancy:
1.
Gestational diabetes 2.preeclampsia
men’s health:
1.
Erectile dysfunction 2. Low testosterone
psychiatry:
1.
Anxiety 2.depression
and pediatric growth and development topics are required:
1.
Giantism 2. pubertal delay
……………………………………………………………………………………………………..
From each of the diseases listed above include:
· Information on the disease/Condition
· What causes it
· Signs and symptoms
· How it is diagnosed
· Common treatment
Each disease is individual, this is NOT a compare between the diseases under the body systems.
………………………………………………………………………………………………
REQUIREMENTS
APA format
15-18 pages
Scholarly articles for sources ONLY!! From years 2015 -2020 only.
.
Pick only one topic!!!!!!!!!!You will need to choose one topic f.docxJUST36
Pick only one topic!!!!!!!!!!
You will need to choose one topic from the following list, explore online resources, and write a report about the topic of your choosing from the following list of topics:
• Disposal of hazardous San Francisco Bay dredging materials
• Earthquake liquefaction hazards around the Bay Area
• Planning for sea level rise around the Bay Area
• Bay Area wetlands restoration projects: past, present and future
• Impacts of filling historical wetlands around the Bay Area
• Stormwater pollution prevention around the Bay Area
• Oil spill hazard mitigation in the San Francisco Bay
• Wastewater pollution prevention around the Bay Area
• Upstream dam construction effects on the estuary health
Lab 3 is asking you to investigate one of the many topics, or issues, related to the San Francisco Bay Estuary and it's restoration. Your deliverable for this assignment is a 1,000 word (at minimum) essay that has AT LEAST five references. The format of your essay should follow the structure outlined in the grading rubric at the end of the assignment sheet (i.e. it should have an Introduction section, Discussion section, and Conclusion section).Please make sure that your paper follows this format, contains at least FIVE references, and has a word count of at least 1,000.
You are required to reference a minimum of five (5) credible sources and include a references section. In addition to a references section, be sure you use intext citations to these sources as their information comes up in your paper.
AND MOST IMPORTANT THING IS NO PLAGIRISM.
Here are some useful information.
https://www.kcet.org/redefine/a-look-at-the-deltas-tastiest-invasive-species
https://www.nationalgeographic.com/news/2016/12/estuaries-california/
http://www.resilientbayarea.org/
https://youtu.be/clZz2OjE5n0
https://youtu.be/dAul4-vE5TM
https://youtu.be/SsxQMgKnClY
Practicum Experience Time Log and Journal Template
Student Name:
E-mail Address:
Practicum Placement Agency's Name:
Preceptor’s Name:
Preceptor’s Telephone:
Preceptor’s E-mail Address:
(Continued next page)
Time Log
Learning Objective
Psychotherapy with Trauma
List AND COMPLETE the 5 objective(s) met and Briefly Describe 8 the Activities you completed during each time period. If you are not on-site for a specific week, enter “Not on site” for that week in the Total Hours for This Time Frame column. Journal entries are due in Weeks 4, 8, and 11; include your Time Log with all hours logged (for current and previous weeks) each time you submit a journal entry.
You are encouraged to complete your practicum hours on a regular schedule, so you will complete the required hours by the END of WEEK 11.
Time Log
Week
Dates
Times
Total Hours for This
Time Frame
Activities/Comments
Learning Objective(s) Addressed
Assess clients presenting with posttraumatic stress disorder
Analyze therapeutic approaches for treating clients presenting with posttraumatic stress disorder
Ev.
Pick one organized religion to research. First, describe the religio.docxJUST36
Pick one organized religion to research. First, describe the religion’s prevalence in the U.S. and membership patterns. Then, apply the symbolic interactionist perspective to this system, describing the symbols, rituals, beliefs, and religious experiences members share. You are required to source your content on this topic.
.
Pick one of the 2 (Buddhist Syllogism or Meditation)...The B.docxJUST36
Pick one of the 2 (Buddhist Syllogism or Meditation)...
The Buddhist Syllogism:
1. “Good” is a judgment.
2. Judgments are a form of attachment.
3. Attachments are the source of all misery and pain.
4. Nirvana is release from all misery and pain through the practice of non-attachment.
5. So
Nirvana is bliss.
6. But if "good" is a judgement and judgements are a form of attachment, and attachments are the source of all misery then
those who say Nirvana (or bliss)
is good
thereby prevent themselves from attaining it
7. So
you must not believe that nirvana is not good....OR you must not want to be in a state of enlightenment.... OR you must not prefer bliss to pain....
Attainment of Nirvana is impeded by desire to attain it. If you want to be without suffering, you will suffer. How, then, does one attain Nirvana?
Above is a traditional discussion on the nature of Nirvana (the ultimate goal of Buddhism.) For this discussion board state why you agree or disagree with the above assessment of the Nature of Nirvana.
Meditation
Meditation is one means of practicing non-attachment, leading to enlightenment.
In some traditions a first step in learning meditation is learning to distinguish the receptive mind from the reactive mind. In meditation, primacy is given to the receptive mind. Reactive states are not to be reacted to, but received. The habitual awareness and non-attachment that result from this practice is called “mindfulness”.
In the meditation drama below, which response is the best example of mindfulness? Why?
Breathe in. Breathe out. Breathe in. Breathe out. Breathe in. Breathe out. I’d kill for a Big Mac. Breathe in.
Responses:
(a) Damn! My mind is so unruly. I’ll never get it under control.
(b) What kind of Buddhist gets distracted by McDonald’s? How embarrassing.
(c) Ah, wishing. It is so hard to stay focused.
(d) Impermanence is the nature of all things. The satisfaction from a Big Mac is fleeting. Your goal is eternal bliss.
(e) None of the above is mindful. A better response would be:
taken from
Spot PCC.edu (Links to an external site.)
Your initial response should be clear and support your view. Write about in your initial post with a minimum length of 175 words.
No References
.
Pick one of the following terms for your research Moral philosophy,.docxJUST36
Pick one of the following terms for your research: Moral philosophy, justice, white-collar crime, differential association, or power.
( DEFINITION: a brief definition of the key term followed by the APA reference for the term; this does not count in the word requirement. SUMMARY: Summarize the article in your own words- this should be in the 150-200 word range. Be sure to note the article's author, note their credentials and why we should put any weight behind his/her opinions, research or findings regarding the key term.
DISCUSSION: Using 300-350 words, write a brief discussion, in your own words of how the article relates to the selected chapter Key Term. A discussion is not rehashing what was already stated in the article, but the opportunity for you to add value by sharing your experiences, thoughts and opinions. This is the most important part of the assignment.
REFERENCES: All references must be listed at the bottom of the submission--in APA format. )
.
The Indian economy is classified into different sectors to simplify the analysis and understanding of economic activities. For Class 10, it's essential to grasp the sectors of the Indian economy, understand their characteristics, and recognize their importance. This guide will provide detailed notes on the Sectors of the Indian Economy Class 10, using specific long-tail keywords to enhance comprehension.
For more information, visit-www.vavaclasses.com
Palestine last event orientationfvgnh .pptxRaedMohamed3
An EFL lesson about the current events in Palestine. It is intended to be for intermediate students who wish to increase their listening skills through a short lesson in power point.
Unit 8 - Information and Communication Technology (Paper I).pdfThiyagu K
This slides describes the basic concepts of ICT, basics of Email, Emerging Technology and Digital Initiatives in Education. This presentations aligns with the UGC Paper I syllabus.
This is a presentation by Dada Robert in a Your Skill Boost masterclass organised by the Excellence Foundation for South Sudan (EFSS) on Saturday, the 25th and Sunday, the 26th of May 2024.
He discussed the concept of quality improvement, emphasizing its applicability to various aspects of life, including personal, project, and program improvements. He defined quality as doing the right thing at the right time in the right way to achieve the best possible results and discussed the concept of the "gap" between what we know and what we do, and how this gap represents the areas we need to improve. He explained the scientific approach to quality improvement, which involves systematic performance analysis, testing and learning, and implementing change ideas. He also highlighted the importance of client focus and a team approach to quality improvement.
The Art Pastor's Guide to Sabbath | Steve ThomasonSteve Thomason
What is the purpose of the Sabbath Law in the Torah. It is interesting to compare how the context of the law shifts from Exodus to Deuteronomy. Who gets to rest, and why?
Read| The latest issue of The Challenger is here! We are thrilled to announce that our school paper has qualified for the NATIONAL SCHOOLS PRESS CONFERENCE (NSPC) 2024. Thank you for your unwavering support and trust. Dive into the stories that made us stand out!
The French Revolution, which began in 1789, was a period of radical social and political upheaval in France. It marked the decline of absolute monarchies, the rise of secular and democratic republics, and the eventual rise of Napoleon Bonaparte. This revolutionary period is crucial in understanding the transition from feudalism to modernity in Europe.
For more information, visit-www.vavaclasses.com
Model Attribute Check Company Auto PropertyCeline George
In Odoo, the multi-company feature allows you to manage multiple companies within a single Odoo database instance. Each company can have its own configurations while still sharing common resources such as products, customers, and suppliers.
We all have good and bad thoughts from time to time and situation to situation. We are bombarded daily with spiraling thoughts(both negative and positive) creating all-consuming feel , making us difficult to manage with associated suffering. Good thoughts are like our Mob Signal (Positive thought) amidst noise(negative thought) in the atmosphere. Negative thoughts like noise outweigh positive thoughts. These thoughts often create unwanted confusion, trouble, stress and frustration in our mind as well as chaos in our physical world. Negative thoughts are also known as “distorted thinking”.
PATIENT FILE151PATIENT FILEThe Case The scatter-b.docx
1. PATIENT FILE
151
PATIENT FILE
The Case: The scatter-brained mother whose daughter has
ADHD, like
mother, like daughter
The Question: How often does ADHD run in families?
The Dilemma: When you see a child with ADHD should you
also
evaluate the parents and siblings?
Pretest Self Assessment Question (answer at the end of the
case)
Patients with comorbid ADHD and anxiety should in general not
be
prescribed stimulants
A. True
B. False
Patient Intake
• 26-year-old woman
• Has a daughter with ADHD
• Psychiatrist noted symptoms in the mother and suggested she
come
2. in for her own evaluation
• See the previous Case 13, p 133 for presentation of the
daughter’s
case
Psychiatric History
• During interviews with the patient’s daughter (also attended
by the
patient) over the past several months, it was not only noted that
the
daughter has ADHD with comorbid ODD, but that the mother
also
exhibited multiple symptoms consistent with lifelong and
undiagnosed
ADHD including
– Mother misses appointments or is late for appointments
– Often appears disorganized
– Did not fi ll out her child’s forms on time
– Did not deliver forms to her child’s teacher, forgot, lost them
– Admits being very disorganized since her second child
started
school
– Feels overwhelmed by two children and her life
circumstances
– Could also have some signs of depression
– Can’t get organized to take her child to CBT
– Has a hard time keeping a regular schedule and also keeping
her
daughter on a regular schedule of going to bed and waking up
– Was unable to remember to remove the daughter’s skin patch
4. both
parents have ADHD and thus was asked to fi ll out an Adult
ADHD
screening form
Social and Personal History
• High school drop out, age 17 after getting pregnant
• Married age 17, divorced 2 years later
• Two children, ages 8 and 6
• Smoker
• No drug or alcohol abuse
• Single mother works full time in retail
• Father not much involved with his children
Medical History
• None notable
• BP normal
• BMI normal
• Normal lab tests
Family History
• 8-year-old daughter: recently diagnosed with ADHD
• Other family history unknown as the patient was adopted
• See the previous Case 13, p 133 for presentation of the
daughter’s
case
Patient Intake
• The last time the patient brought her child to see the
psychiatrist, the
mother was asked to fi ll out her own checklist, the Adult
ADHD Self
Report Scale Symptom Checklist
6. – Her teachers had commented on some of the problems
endorsed
in the adult ADHD checklist that she continues to experience as
an
adult
• Asked how these problems affect her life, she states that:
– They cause great diffi culty managing family matters
– She used to be unable to stay focused in conversations with
her
ex-husband, which made him feel she did not care about him
• Additional complaints include:
– Constantly feeling overwhelmed with taking care of the two
children while working fulltime
– Blaming herself for her daughter’s academic diffi culties
– Feeling very emotional and overwhelmed
– “I’m sorry, doctor, but two kids are just too much for this
single
mom”
• Having diffi culty sleeping and being irritable with the
children at night,
which she regrets later on
• Has many worries, about fi nances, about the future, about her
children’s futures, about getting a better job, about getting her
own
education, about fi nding a new partner
Based on just what you have been told so far about this
patient’s history
8. – Irritability
– Trouble sleeping
• Most adults with ADHD are comorbid for a second psychiatric
disorder, and the most common is GAD
• Also, this patient is a smoker which may be related to her
ADHD
since a disproportionate number of ADHD patients smoke,
perhaps
because of the therapeutic effects of nicotine on ADHD
symptoms
How would you treat her?
• Stimulant for her ADHD
• SSRI/SNRI for her GAD
• Benzodiazepine as need for GAD and insomnia
• Stimulant plus an SSRI/SNRI or benzo for both ADHD and
GAD
• CBT for both ADHD and GAD
• Other
Attending Physician’s Mental Notes, Initial Psychiatric
Evaluation, Continued
• It seems as though the primary disorder is ADHD and it will
be
simplest if this is treated fi rst, with a single drug, probably a
stimulant
• An SSRI/SNRI and/or benzodiazepine can be added at a later
time
once the actions of the stimulant are evident
• Even though patients with GAD alone or even normal controls
may be
10. CBT
session, she had already been titrated to 20 mg of mixed salts of
d,l –
amphetamine XR
• She thought that the medication had already started to help her
and
in fact that she would not have been able to cooperate with the
CBT
assignments had she not been on the medication
• Because of lack of side effects but continuing ADHD and
GAD
symptoms, the dose of d,l-amphetamine XR increased to 30 mg
(off
label since the maximum approved dosage for adults is 20 mg)
• Her BP and pulse were stable on the 30 mg dose but she felt
jittery
particularly in the morning and around noon; she also felt very
anxious
about her job situation and being able to provide for her family
• Dose lowered to 25 mg, but the jitteriness persisted so the
dosage
was further lowerd to 20 mg
• The jitteriness abated but her ADHD symptoms were not well
controlled on the 20 mg dose anymore
• Instructed to stay on 20 mg for two more weeks as she is
going on
vacation and not to change the dose until after her vacation and
then
retry the 25 mg dose again
11. • Complained of feeling overwhelmed and irritable
• For most patients, a week between dosing adjustments for a
stimulant
being used to treat ADHD is quite adequate
• Weekly intervals give patients and clinicians a chance to see
the way
that the dosage is working though the spectrum of challenges
that
occur in a typical week
• As vacations do not represent typical activities for a week,
special
consideration must be given to the effectiveness of medication
changes that are done while a patient is on vacation
– Many adults with ADHD may relax on vacation and not
challenge
themselves with cognitive loads and multitasking so may appear
to be better even without a medication change
– Other adults with ADHD, especially women with young
children,
may actually fi nd vacation more challenging
– For example, a parent with ADHD taking a family vacation
with
several children in tow may fi nd the planning and organization
for
the trip more taxing than anything encountered at work or
during
the normal routine at home
– It can also be diffi cult to manage timing the medication
13. really
helping her concentrate and get through the day even though she
remains symptomatic
• Knowing that she could achieve better functioning on
medication she
asked if other medications might accomplish this without the
jittery
and anxious feelings
• While other medication options were discussed, the CBT was
continued which was slightly less helpful
How would you treat her now?
• Start lisdexamfetamine 30 mg once in the morning and titrate
the
dosage by 20 mg each week until an optimal dosage is achieved
• Start d-methylphenidate XR 10 mg once in the morning and
titrate the
dosage by 10 mg each week until an optimal dosage is achieved
• Start OROS methylphenidate 18 mg once in the morning and
titrate
the dosage by 18 mg each week until an optimal dose is
achieved
• Start atomoxetine 40 mg a day and increase to 80 mg after one
week
Attending Physician’s Mental Notes: Fourth Interim Followup,
Week 16
• Lisdexamfetamine, d-methylphenidate XR, OROS
methylphenidate,
15. • Methylphenidate LA and d-methylphenidate XR employ the
same
patented SODAS technology in their delivery systems, but other
long-
acting forms of stimulants with beaded delivery systems vary
due to
proprietary differences in their manufacturing processes
• For instance, one formulation of methylphenidate utilizes a
capsule
that contains a ratio of 30 percent immediate-release beads and
70
percent delayed-released beads
• Although the different technologies used in beaded forms of
stimulants can have clinical implications in individual cases,
they all
follow a similar design scheme:
– A bolus of stimulant medication becomes bioavailable rather
quickly as the immediate-release beads dissolve
– Over time, the coating on the delayed-release beads
deteriorates,
allowing the stimulant contained within the bead to be released
– The medication within the delayed-release bead becomes
bioavailable about four hours after the patient swallows the
capsule
• Lisdexamfetamine is the only stimulant preparation that is a
prodrug:
– In its prodrug form, a lysine molecule is attached to
dextroamphetamine
– Dextroamphetamine will not be active until the lysine is
16. cleaved
from it
– Cleaved lysine is an amino acid that does not contribute to
the
clinical effi cacy of this medication
• Lisdexamfetamine could be a good choice for multiple
reasons:
– It uses a different delivery system that appears to have a
more
consistent interval to maximum concentration (Cmax)
• It is conceivable that the jitteriness this patient was
experiencing was
related more to the l-isomer than to the d-isomer
• A nonstimulant such as atomoxetine may be particularly useful
in a
patient who has stimulant related side effects, because
atomoxetine
does not cause these side effects
• Also, atomoxetine may be particularly useful in patients with
comorbid anxiety
Case Outcome: Fourth Interim Followup, Week 16, Continued
• In the end, the patient and the attending physician agreed upon
a trial
of OROS methylphenidate (Concerta)
• Main reasons for this choice:
– To be able to compare the benefi ts the patient experienced
on
18. – A push compartment absorbs water and expands like a sponge
does, pushing the methylphenidate gel out of the hole at the
opposite end
Case Outcome: Fifth Interim Followup, Week 20
• The patient’s dose was titrated from 18 mg to 72 mg over the
course
of four weeks
• Although she did not feel jittery, OROS methylphenidate 72
mg once a
day did not seem to work as well as the mixed salts
amphetamine at
30 mg a day
• She voiced concerns that the dosage was more than double that
of
the mixed salts amphetamine dosage that was tried
• The psychiatrist explained that methylphenidate compounds
are half
as potent as amphetamine ones, and that 72 mg/day is an
approved
dose in adults
• She was reminded that her blood pressure and pulse had
remained
in the normal range throughout the titration, and she was told
that
some of the methylphenidate gel may remain inside the delivery
system and not be bioavailable (inherent proper ties of OROS
technology)
• After documenting that information about off-label use was
20. – “It’s like now that I can concentrate on my daily tasks, I also
feel
much more anxious about the fi nancial security of my children,
and I often feel my throat tighten when I think about the fi
nancial
impact of the girls going to college”
– “The thought of losing my job or getting sick frightens me . .
.
what would happen to the girls?”
– She has trouble falling asleep at night, as her mind does not
shut
off
ADHD is often comorbid with other psychiatric disorders and
one
disorder can mask the symptoms of another. In the present case,
this
patient exhibits symptoms of anxiety, probably generalized
anxiety
disorder, especially more prominent every time her ADHD
symptoms
abate. How would you address the patient’s anxiety at this
point?
• Augment with a benzodiazepine
• Augment with buspirone
• Augment with a selective serotonin reuptake inhibitor (SSRI)
or SNRI
• Incorporate techniques to resolve anxiety into ongoing CBT
21. Case Outcome: Seventh and Eighth Interim Followup, Weeks
24 and 36
• Incorporating techniques to resolve anxiety into the patient’s
ongoing
CBT would likely be most appropriate, prior to attempting to
add a
medication
• A letter was sent suggesting this to the CBT therapist, but
after 12
weeks, this led to limited benefi t, and thus medication
augmentation
was considered
• Benzodiazepines, buspirone, and SSRIs/SNRIs can all be used
to
treat generalized anxiety disorder and are not contraindicated
with
stimulants
• After discussion of the options, paroxetine was prescribed to
augment
her stimulant and her CTB
Case Outcome: Ninth Interim Followup, Week 48
• After three months on OROS methylphenidate and paroxetine,
while
continuing her CBT, at fi rst the patient stated that she “had her
life back”
• Then, after thinking back over the past year of treatment, and
to how
she had been since childhood she stated, “No, I don’t have my
life
23. recognize their own symptoms once their child is diagnosed
• A multigenerational approach should be considered for parents
who
have ADHD and who care for children with ADHD
• In the patient’s case, by addressing her own ADHD issues, she
also
felt she could be a better parent to her daughter with ADHD
Performance in Practice: Confessions of a
Psychopharmacologist
• What could have been done better here?
– Perhaps ADHD could have been recognized earlier
– Perhaps CBT could have been implemented earlier
– Perhaps she should have been more actively engaged or have
had
more serious discussions about smoking cessation already
• Possible action item for improvement in practice
– Make a concerted effort to keep contact with low cost CBT
resources in the community
– Make a more concerted effort to encourage smoking cessation
Tips and Pearls
• Prescribing stimulants to an ADHD patient is very much like
tailoring a
“bespoke” treatment, one case at a time
• That is, some patients respond very differently to
amphetamine than
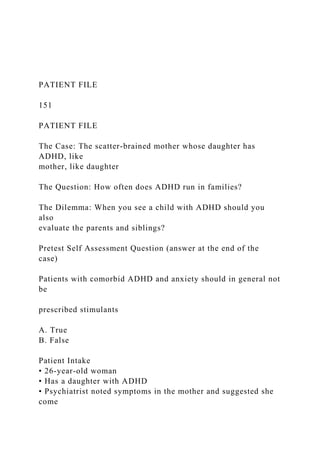
26. ADHD is one of the most genetically loaded medical or
psychiatric
conditions, higher than schizophrenia, asthma or breast cancer.
Posttest Self Assessment Question: Answer
Patients with comorbid ADHD and anxiety should in general not
be
prescribed stimulants
A True
B False
Answer: B
References
1. Franke B, Neale BM, and Faraone SV. Genome-wide
association
studies in ADHD. Hum Genet 2009; 126(1): 13–50
2. Haberstick BC, Timberlake D, Hopfer CJ et al. Genetic and
environmental contributions to retrospectively reported DSM-IV
childhood attention defi cit hyperactivity disorder. Psychol Med
2008;
38(7): 1057–66
3. McLoughlin G, Ronald A, Kuntsi J et al. Genetic support for
the
dual nature of attention defi cit hyperactivity disorder:
substantial
genetic overlap between the inattentive and hyperactive-
impulsive
components. J Abnorm Child Psychol 2007; 35(6): 999–1008
4. Todd RD, Rasmussen ER, Neuman RJ et al. Familiality and
27. heritability of subtypes of attention defi cit hyperactivity
disorder in
a population sample of adolescent female twins. Am J
Psychiatry
2001; 158(11): 1891–8
5. Faraone SV, Advances in the genetics and neurobiology of
attention
defi cit hyperactivity disorder, Biol Psychiatry 2006; 60: 1025–
7
Twin studies: ADHD is genetic
Hudziak, 2000
Nadder, 1998
Levy, 1997
Sherman, 1997
Silberg, 1996
Gjone, 1996
Thapar, 1995
Schmitz, 1995
Edelbrock, 1992
Gillis, 1992
Goodman, 1989
Willerman, 1973
Breast cancer Asthma Schizophrenia Height
Average genetic contribution of ADHD based on twin studies
ADHD