
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Mastoid surgeries KK .ppt
Similar to Mastoid surgeries KK .ppt (20)
More from DrKrishnaKoiralaENT
More from DrKrishnaKoiralaENT (20)
Recently uploaded
Recently uploaded (20)
Mastoid surgeries KK .ppt
- 1. Dr. Krishna Koirala // Mastoid Surgeries
- 2. • Surgery performed on the mastoid to remove disease from the mastoid bone Classification A. According to the status of bony canal wall − Canal Wall up (bony canal wall is kept intact) • Cortical • Combined Approach Tympanoplasty (CAT) − Canal Wall down (bony canal wall is broken down) • Atticotomy • Modified Radical / Radical mastoidectomy
- 3. B. According to extent of soft tissue/bone removal − Cortical Mastoidectomy − Modified Radical / Bondy’s mastoidectomy − Radical Mastoidectomy
- 4. • To make ear safe by eliminating cholesteatoma, granulations and chronic infection • To make the ear problem-free for all usual activities of daily living, including swimming • To restore or improve hearing whenever possible • To provide an acceptable cosmetic appearance
- 5. • Approaches to Mastoid Surgeries – End aural (Lempert’s) – Postaural (Wilde’s) – Extended Endaural – Circumferential
- 6. • Advantages − Normal appearance of EAC − Hearing aids easily fit − No routine cleaning required − High tolerance for water exposure • Disadvantages − Usually a staged procedure − Relatively high rate of recurrent or persistent cholesteatomas
- 7. • Advantages − Usually a single procedure − Low rate of persistent or recurrent cholesteatomas • Disadvantages − Enlarged external auditory meatus − Hearing aids difficult to fit − Periodic canal cleaning needed − Occasional problem with water exposure
- 8. • Synonyms −Schwartz's operation −Simple mastoidectomy −Complete mastoidectomy
- 9. − Complete exenteretion of all accessible mastoid air cells and convert them into a single cavity − Posterior canal wall and middle ear structures kept intact
- 10. • Incompletely resolved ASOM with reservoir sign • CSOM TT not responding to conservative medical treatment • Acute coalescent mastoiditis • Masked Mastoiditis • Approach to − Endolymphatic sac surgery − Facial nerve decompression − CP angle tumors (Translabyrinthine approach) − Cochlear implant surgery
- 11. • Wilde’s Postauricular incision • Dissection of soft tissues and preparation of graft • Elevation of periostium • Identification of MC Ewan's triangle • Exposure of Mastoid antrum • Exenterating of all accessible mastoid air cells • Placement of graft • Placement of drain • Closure of wound and mastoid dressing
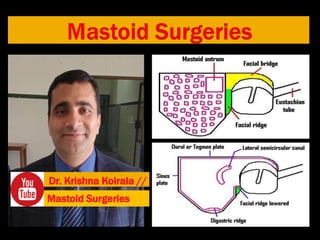
- 15. • Superior : Dural plate • Inferior : Digastric ridge • Anterior : Posterior wall of external auditory canal • Posterior : Sigmoid sinus plate • Medially : Dome of Lateral semicircular canal
- 16. • An operation performed to eradicate disease from the middle ear cavity and mastoid , in which the mastoid and epitympanic spaces are converted into an easily accessible common cavity by removing the posterior and superior external bony canal walls with preservation of the healthy ossicles and TM remnant
- 17. • Aim − Eradicate disease from the middle ear cleft in order to make the ear safe and dry and to preserve or improve hearing • Indications – CSOM AA with adequate cochlear function (serviceable hearing)
- 18. • All accessible diseased mastoid air cells along with cholesteatoma and granulations are removed • Bony posterior canal wall is lowered • Disease from the middle ear cavity is removed but normal mucosa of middle ear, remnant TM and healthy ossicles are preserved • Mastoid cavity and EAC become a single cavity separated by middle ear cavity
- 19. Perform Tympanoplasty and concho - meatoplasty Preserve healthy mucosa, T.M. remnant and ossicles Remove cholesteatoma and granulations from mastoid air cells & middle ear cavity Lower facial ridge and break facial bridge Perform cortical mastoidectomy
- 20. A large, adequate meatoplasty is necessary to create a problem-free cavity
- 21. • Aims − Remove / eradicate disease from the middle ear cleft − Make the ear safe and dry − No attempt made to preserve hearing
- 22. 1. CSOM atticoantral disease with − Profound sensorineural hearing loss − Intra-cranial complication − Recurrence after modified radical mastoidectomy 2. Limited malignancy of middle ear 3. Glomus jugulare 4. Osteomyelitis of temporal bone
- 23. − All accessible diseased mastoid air cells along with cholesteatoma and granulations are removed − Bony posterior canal wall is lowered down − Disease from the middle ear cavity along with the mucosa of middle ear, remnant TM and ossicles except the stapes footplate are removed − Eustachian tube opening is closed and mastoid cavity , EAC and middle ear cavity all are converted to a single cavity
- 24. • Perform cortical mastoidectomy • Lower facial ridge & break facial bridge, remove cholesteatoma & granulations from mastoid air cells & middle ear • Remove remnant middle ear mucosa, T.M. remnant & ossicles (except stapes footplate) • Close Eustachian tube opening and perform Concho - meatoplasty • Mastoid, E.A.C. & middle ear become single cavity
- 25. • Injury to dural plate leading t bleeding, CSF leak and brain fungus • Injury to the sigmoid sinus leading to bleeding • Injury to facial nerve leading to complete or incomplete facial palsy • Injury to the stapes footplate leading to sensorineural hearing loss/ dead ear • Incomplete surgery leading to residual disese • Mastoid cavity problems in including discharging mastoid cavity
- 26. 1. Inadequate concho-meatoplasty 2. Recurrence of cholesteatoma 3. Residual cholesteatoma in : Facial ridge, sinodural angle , mastoid tip, sinus tympani, anterior Epitympanum 4. Persistent infection : Petrositis, T.B., sinusitis 5. Persistent allergy 6. Retained foreign body : cotton ball 7. Wrong indication
- 27. Mastoid cavity problems can be reduced by • Complete removal of disease • Saucerization of cavity • Adequate lowering of facial ridge • Round cavity • Wide conchomeatoplasty • Grafting the tympanic membrane
- 28. • Advantages − Faster healing − Easier long-term postoperative care − No water precautions necessary (particularly important in children and water sports) − More options available for hearing aid, if necessary • Disadvantages − Epitympanum /mastoid not accessible to post operative inspection − Supratubal space not easily accessible unless malleus head and incus removed − Both residual and recurrent disease more likely − Greater number of procedures required for disease eradication
- 29. • Cortical Mastoidectomy • Anterior Tympanotomy via tympano-meatal flap • Posterior tympanotomy via facial recess • Tympanoplasty