Downloaded 14 times

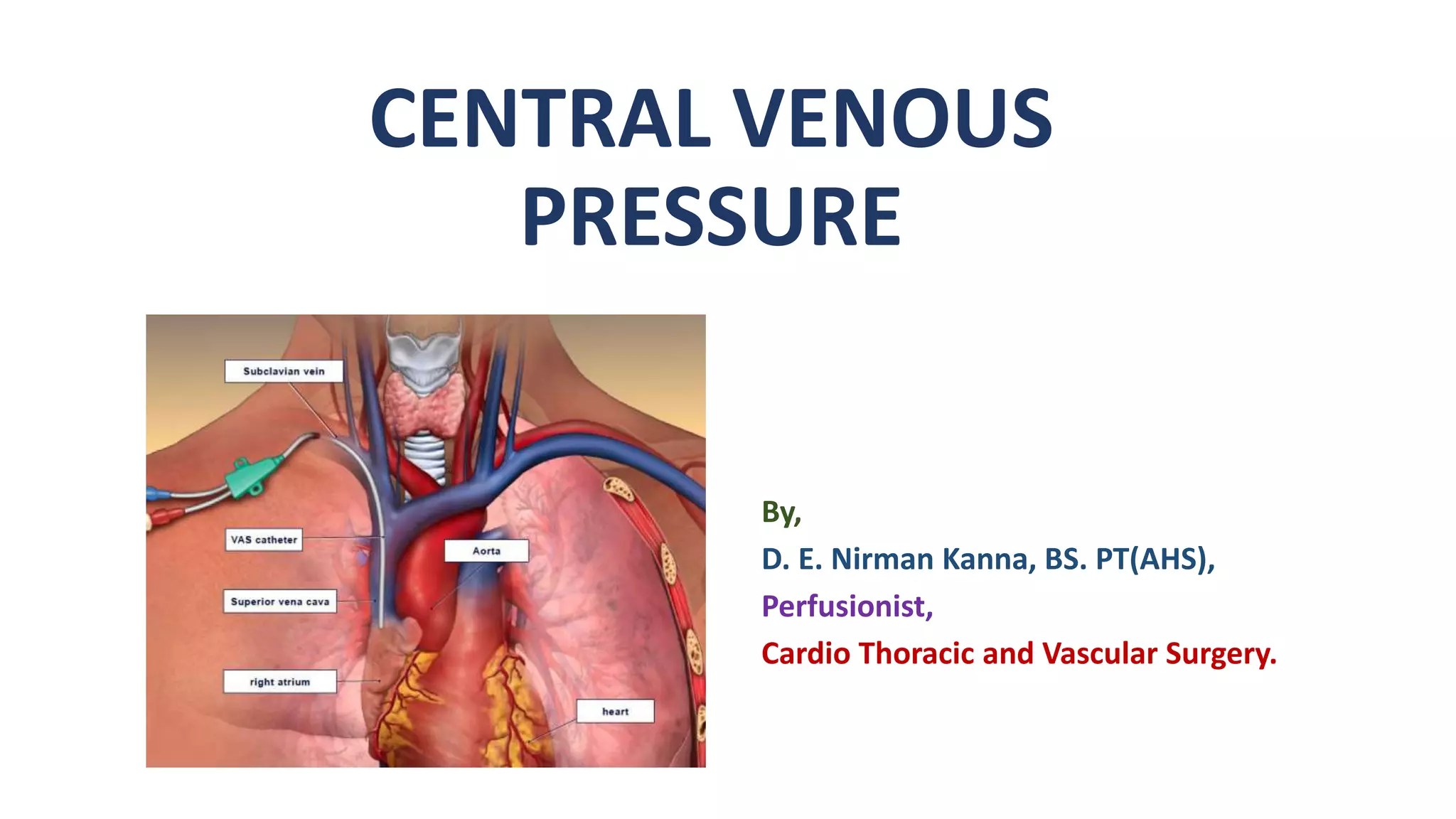
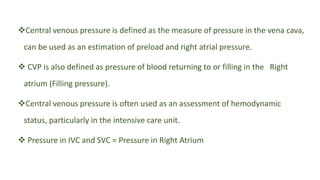
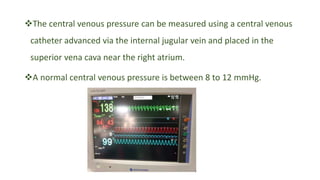
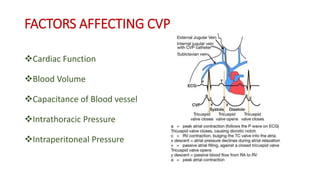

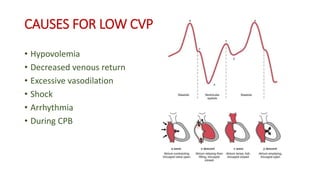
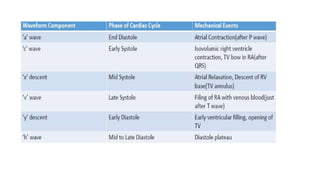
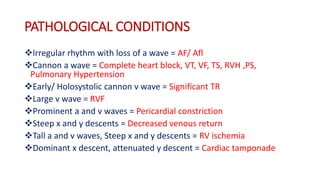

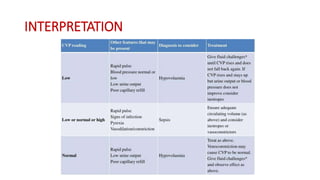

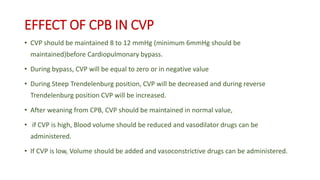


Central venous pressure (CVP) measures pressure in the vena cava, reflecting preload and right atrial pressure, and is crucial in assessing hemodynamic status in critical care. Normal CVP is between 8 to 12 mmHg and can be affected by factors such as cardiac function and blood volume; various causes for high or low CVP are identified. Additionally, CVP readings, along with their waveform patterns, provide insights into possible pathological conditions during procedures like cardiopulmonary bypass.




















































![Principles of Valve Sparing Procedure [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/principlesofvalvesparingprocedureautosaved-240916162853-74278697-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)