
More Related Content
What's hot
What's hot (20)
Similar to Hydrocephalus.pdf
Similar to Hydrocephalus.pdf (20)
More from Shapi. MD
More from Shapi. MD (20)
Recently uploaded
Recently uploaded (20)
Hydrocephalus.pdf
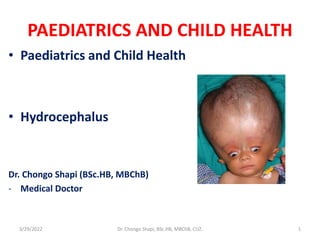
- 1. PAEDIATRICS AND CHILD HEALTH • Paediatrics and Child Health • Hydrocephalus Dr. Chongo Shapi (BSc.HB, MBChB) - Medical Doctor 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 1
- 2. 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ 2
- 3. 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 3
- 4. Hydrocephalus • Is the disturbance of CSF formation, flow or absorption leading to an abnormal accumulation of CSF in the ventricles of the brain • Is classified according to its underlying pathology • It can be classified into: 1. Communicating hydrocephalus (non-obstructive): no obstruction 2. Non-communicating (obstructive) hydrocephalus: where there is obstruction - Can also be classified into congenital or acquired hydrocephalus 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ 4
- 5. Communicating hydrocephalus - No reabsorption of CSF into the dural venous sinuses - Can occur with subarachnoid haemorrhage (SAH) or congenital absence of arachnoidal granulation - This results in accumulation of CSF within the subarachnoid space causing compression of the brain tissue within the cranial cavity - This leads to brain atrophy and long-term mental retardation 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 5
- 6. CT scan See the progression 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 6
- 7. Non-communicating Hydrocephalus • There is usually blockage within the ventricular system • This results in accumulation of CSF within the ventricular system • The brain matter therefore is pushed outwards against the skull 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 7
- 8. Causes of Non-Communicating Hydrocephalus 1. TORCHES 2. Mass lesions: abscess, haematoma, tumours 3. Aqueductal stenosis 4. Dandy Walker Malformation (DWM): - Prominent occiput due to cystic expansion of the 4th ventricle in the posterior cranial fossa and midline cerebellar hypoplasia resulting from developmental failure of the 4th ventricle during embryogenesis 5. Anold Chiari Malformation type II (ACM-II): - For-shortened occiput where portions of the cerebellum and brainstem herniate into the cervical spinal canal blocking CSF flow to posterior cranial fossa 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ 8
- 9. Causes of Communicating Hydrocephalus 1. Meningitis (TB) 2. Subarachnoid haemorrhage (SAH) 3. Meningeal malignancy 4. Absence of arachnoid granulations 5. Choroid plexus papilloma 6. Basilar impression 7. Achondroplasia (due to increased dural venous sinus pressure) 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ 9
- 10. Questions to Establish Diagnosis Perinatal: - Was the child born at term or preterm? - Did the child cry immediately after birth? - What was the head circumference at birth? - Any abnormality of the spine? Post-natal: • At what age did the caregiver notice the head getting bigger? • Did the child have any fever before the head started getting big? • What treatment was given and for how long? • Any history of convulsions? • Any similar illness in the siblings? 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 10
- 11. Clinical Presentation SYMPTOMS • Infants: - Poor feeding - Irritability - Reduced activity - Vomiting • Children and adults include the following: - Cognitive deterioration - Headaches (initially in the morning) - Neck pain, suggesting tonsillar herniation - Vomiting, more significant in the morning - Blurred vision: A consequence of papilledema and, later, of optic atrophy - Double vision: Related to unilateral or bilateral sixth nerve palsy - Difficulty in walking due to spasticity: more in lower limbs because the periventricular pyramidal tract is stretched by the hydrocephalus - Drowsiness 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ 11
- 12. SIGNS Infants: • Head enlargement (head circumference ≥98th percentile for age) • Separation (dysjunction) of sutures • Dilated scalp veins • Delayed closure of anterior fontanelle and will be tense • Sun-setting eye sign: - Characteristic of increased intracranial pressure (ICP); downward deviation of ocular globes, retracted upper lids, visible white sclerae above iris - Increased limb tone (spasticity preferentially affects the lower limbs) 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 12
- 13. 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 13
- 14. 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ 14
- 15. Children and adults: • Papilledema • Failure of upward gaze • Unsteady gait • Large head • Unilateral or bilateral sixth nerve palsy (secondary to increased ICP) 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 15
- 16. Work UP • Lab - No specific blood tests are recommended - Genetic testing and counselling when X-linked hydrocephalus is suspected - Evaluate CSF in post-hemorrhagic and post-meningitic hydrocephalus to exclude residual infection • Imaging - Skull X-ray (calcifications, thin skull bones, separation of sutures, beaten copper appearance (BCA)) - CT/MRI head - EEG when seizures 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ 16
- 17. Beaten copper appearance 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 17
- 18. Treatment • Surgery is the mainstay of treatment • Medical - Use is controversial - As temporal measure to treat post-hemorrhagic or post-meningitic hydrocephalus in neonates to delay surgical intervention - Medications: a. Decreasing CSF secretion by the choroid plexus - Acetazolamide - Furosemide b. Increasing CSF reabsorption - Isosorbide (effectiveness is questionable) 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 18
- 19. Surgical Treatment • Surgical treatment is the preferred therapeutic option • Options: a. Shunting - Ventriculoperitoneal (VP) - Ventriculoatrial (VA) - Lumboperitoneal - Ventriculopleural - Torkildsen shunt b. Endoscopic third ventriculostomy (ETV) 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 19
- 20. Shunting • The principle of shunting is to establish a communication between the CSF (ventricular or lumbar) and a drainage cavity (peritoneum, right atrium, pleural cavity) • Shunts are not perfect • All alternatives to shunting should be considered first 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 20
- 21. VP shunt • Is used most commonly • The lateral ventricle is the usual proximal location • The advantage of this shunt is that the need to lengthen the catheter with growth may be obviated by using a long peritoneal catheter • This reduces repeated lengthening in a growing child 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ 21
- 22. VA shunt • Also called a "vascular shunt.“ • It shunts the cerebral ventricles through the jugular vein and superior vena cava into the right cardiac atrium • It is used when the patient has abdominal abnormalities: - Peritonitis - Morbid obesity - After extensive abdominal surgery • This shunt requires repeated lengthening in a growing child 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 22
- 23. Lumboperitoneal Shunt • Used only for: - Communicating hydrocephalus - CSF fistula - Pseudotumor cerebri 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ 23
- 24. Torkildsen shunt • Used rarely • It shunts the ventricle to cisternal space • Effective only in acquired obstructive hydrocephalus 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 24
- 25. Ventriculopleural shunt • A ventriculopleural shunt is considered second line due to fear of breathing difficulties • Used if other shunt types are contraindicated 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ 25
- 26. Complications of Shunting 1. Risk of infection 2. Blockage of the shunt 3. Patient outgrows the shunt 4. Shunt dislodgement 5. Shunt nephritis 6. Subdural haematoma 7. Pseudocyst 8. Slit ventrical syndrome due to overdrainage (CT/MRI shows very small “slit-like” collapsed ventricles) 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ 26
- 27. ETV • Is a surgical procedure in which an opening (ostomy) is created in the floor of the 3rd ventricle using an endoscope placed within the ventricular system through a burr hole (trephine) • This allows the CSF to flow directly to the basal cisterns, thereby shortcutting any obstruction • It is used as an alternative to a cerebral shunt to treat certain forms of obstructive hydrocephalus, such as aqueductal stenosis • Complications include subarachnoid haemorrhage, basilar artery injury and hypothalamic or pituitary injury 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 27
- 28. ETV 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ 28
- 29. Thanks 3/29/2022 Dr. Chongo Shapi, BSc.HB, MBChB, CUZ. 29