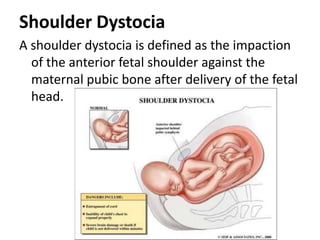
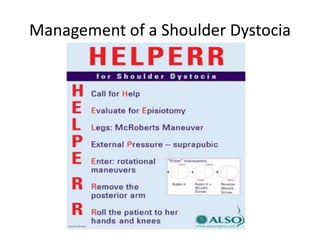
Shoulder dystocia occurs when the baby's shoulder gets stuck behind the mother's pubic bone after the head is delivered. There are no warning signs but risk factors include gestational diabetes, obesity, previous shoulder dystocia, and fetal macrosomia. Signs include a prolonged second stage of labor or the baby's head delivering but the shoulders remaining stuck. Management involves maneuvers like the McRoberts position or suprapubic pressure while last resort maneuvers include breaking the clavicle or performing a symphysiotomy. Thorough documentation is important for teaching, learning, and any potential medical-legal issues.