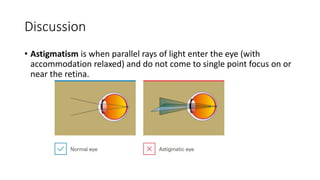
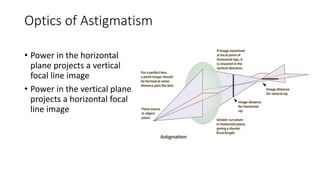
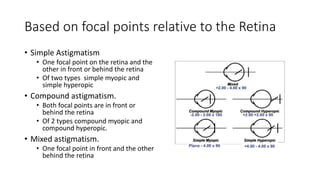
A 36-year-old man presented with complaints of blurry vision when reading or doing near tasks. Examination found compound hyperopic astigmatism. Refraction found +2.00/-1.00X100° in the right eye and +2.25/-1.00X100° in the left eye. Astigmatism is caused by an irregular curvature of the cornea or lens that results in unequal refractive power in different meridians. It is typically treated with spectacles containing cylindrical lenses.