Ophthalmology | Esotropian squint
•
2 likes•322 views

This document discusses esotropia, or convergent strabismus, where the eyes turn inward. It defines strabismus and the different types of eye turns that can occur. It specifically focuses on esotropia, describing the different types including accommodative esotropia caused by hyperopia, non-accommodative esotropia from other causes, and infantile esotropia presenting in the first 6 months of life. It discusses the evaluation and management of esotropia, including correcting refractive errors, treating amblyopia with patching, and considering surgery if needed to align the eyes. The goal of treatment is to improve vision in both eyes and maximize binocular vision.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Ophthalmology | Esotropian squint
Similar to Ophthalmology | Esotropian squint (20)
More from Ali Kareem
Recently uploaded
Recently uploaded (20)
Ophthalmology | Esotropian squint
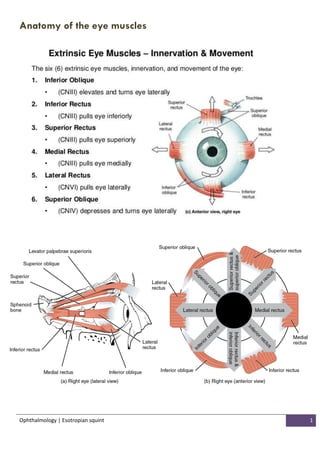
- 1. Ophthalmology | Esotropian squint 1 Anatomy of the eye muscles
- 2. Ophthalmology | Esotropian squint 2 What Is Strabismus? Strabismus is a visual problem in which the eyes are not aligned properly and point in different directions. One eye may look straight ahead, while the other eye turns inward, outward, upward, or downward. The eye turn may be consistent, or it may come and go. Which eye is straight (and which is misaligned) may switch or alternate. Strabismus is a common condition among children. About 4 percent of all children in the United States have strabismus. It can also occur later in life. It may run in families; however, many people with strabismus have no relatives with the problem. What is Squint ? A squint is defined as the inability to make co-ordinated movements of the two eyes, so that the visual axes are not directed simultaneously towards the same fixation point. The squint may be concomitant, where the angle of deviation remains approximately constant in all positions of gaze, or incomitant where the angle varies with the gaze position. Concomitant squints may be subdivided according to whether the visual axes are deviated inwards ("eso" deviations) or outward ("exo" deviations). What is accommodation ? increase in the refractive power of the eye on looking to a near object so that its image is clearly focused on the retina. Accommodation is part of the near reflex, which is initiated by looking to a near object and includes Accommodation Convergence (inward movement of the eyes) Miosis (constriction of the pupil) Normally one dioptre of accommodation is associated with 4 prism dioptres convergence AC/A = 4/1
- 3. Ophthalmology | Esotropian squint 3 amblyopia Amblyopia is a term used to describe loss of visual acuity in an eye without an apparent organic cause. Recent work suggests however that visual deprivation, at least in the developing eye, may result in histological changes in the lateral geniculate body, and the binocularly driven cells of the occipital cortex subsequently respond only to stimuli from the non-amblyopic eye. Convergent concomitant squint - esotropia One eye of a patient may constantly turn inwards while the other eye is used for fixation, and this is called a constant concomitant convergent squint or esotropia (e.g. if the right eye is constantly squinting this is termed a right esotropia). Eso deviations are the most common type of concomitant squint, with the peak incidence of onset between the ages of two-and-a-half and five years.
- 4. Ophthalmology | Esotropian squint 4 If the eyes are used alternately for fixation, this is described as an alternating concomitant convergent squint. The angle of squint may vary with distance, and the variation may be so great that the patient may be binocular at one distance and squint at another distance e.g. straight for distance but convergent for near. Esotropias may be categorised as: 1. accommodative 2. non-accommodative 3. infantile 1. Accommodative esotropia is the most common type of esotropia. It is an esotropia that is produced by or caused by accommodation. Accommodation is always accompanied by convergence, called accommodative convergence. In the normal person, accommodation on a near target produces a convergence of both eyes such that the near target is seen clearly and singly. There is a normal relation between the accommodation on the near target and the accommodative convergence (i.e., normal AC/A ratio). When a normal person who is a little farsighted or hyperopic looks at a distant object, accommodation brings the image of the object of interest to a sharp focus on the retina.there are combinations and variations of these two types. In the more common type, there is a normal AC/A ratio, but the accommodation needed is excessive because of abnormally large hyperopia. This is called the refractive type of accommodative esotropia (Fig. 11.6).
- 5. Ophthalmology | Esotropian squint 5 In the less common type, the accommodation or hyperopia is normal, but the convergence response, the AC/A ratio, is abnormally high. This type may be called the nonrefractive, the high AC/A, or the convergence excess type. The average age of onset for either type of accommodative esotropia is 2.5 years, with a range of 6 months to 6 years of age. When either type begins before 1 year of age, it may be confused with congenital esotropia. 2. Non accommodative esotropia Non accommodative causes of esotropia include stimulus deprivation, divergence insufficiency, consecutive esotropias and stress induced esotropia. Stimulus deprivation esotropia. A squint may result from the reduction of vision in one or both eyes. If the vision is reduced severely by organic ocular or intracranial disease, the binocular reflex is lost and the eye with a poor visual acuity will drift into the anatomical position of rest (either convergent or divergent). Therefore every patient with a squint must be carefully examined to exclude any organic cause reducing the visual acuity (e.g. cataract, retinoblastoma, optic nerve disease). Regrettably cases still occur where the reduced vision in one eye is thought to be due to strabismic amblyopia, and treatment of the real cause is delayed.
- 6. Ophthalmology | Esotropian squint 6 Divergence insufficiency: This squint is the opposite to convergence excess. In this situation the patient is fully binocular for near but exhibits a manifest convergent squint for distance. This is usually due to reduced function of one or both lateral recti and it is important that any underlying sixth nerve palsy is excluded. Consecutive squints: This is a term used to describe the change of a squint from either divergent to convergent or vice versa following surgery to correct the original condition. Consecutive deviations may be present immediately post-operatively or may develop some years after the surgery in a patient who does not have a sufficient degree of binocular vision to hold the eyes straight. The onset of a large consecutive squint immediately after surgery should raise the possibility that one of the muscles operated on has slipped from or become detached from the eye. The tendency is usually towards divergence with the passage of time so that it may sometimes be wise to delay operation for divergent squint in cases with poor binocularity, if cosmetically acceptable. Stress induced squint: Some children who have never demonstrated any tendency to squint may develop a large esotropia acutely following a febrile illness or an accident. Once any underlying neurological defect or refractive error have been excluded, treatment is usually surgical, as there is usually a potential for good binocular function.
- 7. Ophthalmology | Esotropian squint 7 3. Infantile esotropia This is a form of esotropia which presents in the first six months of life, usually with a large convergent squint. The baby cross fixates, using the inturning left eye to look right and vice versa, and this gives the false impression of bilateral sixth nerve palsies. In addition to the esotropia there may also be latent nystagmus , and an upward and outward movement of either eye on occlusion, termed dissociated vertical deviation. After correcting any amblyopia and refractive errors, early surgery is usually recommended, but long term follow up is necessary to avoid amblyopia.
- 8. Ophthalmology | Esotropian squint 8 Management of a child suspected of a convergent squint History An adequate medical history including obstetric and birth history as well as method of delivery is essential. The general progress in achieving developmental milestones, as well as the age of onset of the squint and its duration are important, as is a family history. The chance of regaining binocular vision is better: the later the squint developed, because the binocular reflex is more mature and so more easily restored the sooner the squint is treated after its onset Examination All children with suspected squints should be assessed by an orthoptist, and management planned jointly. During examination of the child the following features should be noted: the appearance of the child. Much information may be gained by watching the patient to assess general health, apparent maturity and any obvious sign of retardation. Epicanthic folds (p462) or broad nasal bridges often give an irresistible impression of convergent squint. Such an 'apparent' or pseudosquint is excluded by subsequent tests. visual acuity and refractive error determination as far as practicable ocular movements in all directions of gaze should be assessed The cover test and the uncover test.
- 9. Ophthalmology | Esotropian squint 9
- 10. Ophthalmology | Esotropian squint 11 The cover test to detect a manifest squint. The patient is asked to look at an object held in the observer's hand. One eye is then covered and the other eye watched to see if it moves to take up fixation. If it moves, it must have previously been deviating. The procedure is then repeated on the other eye. The uncover test to detect a latent deviation. One of the patient's eyes is covered and he is asked to look at an object held by the observer. The eye behind the cover takes up the dissociated position. When the eye is uncovered the movement of the eye to take up fixation is readily detected. The degree of movement reveals the angle of latent squint and the speed of recovery indicates the strength of binocular vision. This is then repeated on the other eye. Rapid movement of the cover between the eyes in the alternating cover test will detect small degrees of latent squint. The cover test and the uncover test must be performed both for distance and near. It is common practice to do a cover test for near with a light, but a target requiring accommodation should be used, such as a small picture or letter.
- 11. Ophthalmology | Esotropian squint 11
- 12. Ophthalmology | Esotropian squint 12 a general ocular examination is important to exclude any abnormalities predisposing to a squint and special care must be taken to detect an afferent pupil defect by the use of the swinging flashlight test. If an afferent defect ispresent it suggests that the low vision may be due to an underlying and possibly serious organic cause. The fundi are examined with the aid of a mydriatic at the time of refraction. cycloplegic refraction. All children with a convergent squint require a refraction under cycloplegia, i.e. with the ciliary muscle paralysed, because their ability to accommodate is so great that a serious underestimate of hypermetropia may otherwise be made. Although atropine is the most effective cycloplegic, because of its potential toxicity it is now used only in special circumstances for children when it is essential to know the full extent of the hypermetropia. It is then used as Oc. atropine 1% twice daily for three days immediately prior to the refraction test. Used in this way toxic effects are rare, but, to prevent systemic absorption, atropine in the form of drops should not be used for this purpose. In most children the use of a short- acting cyclopegic such as cyclopentolate 1% is sufficient. A fundus examination is carried out at the same time as the refraction. Very occasionally a child is unable to cooperate and an examination under an anaesthetic is necessary.
- 13. Ophthalmology | Esotropian squint 13 Treatment of convergent concomitant squint (Esotropia) The aim of treatment is to overcome amblyopia, maximise the degree of binocular single vision and correct the angle of squint. Treatment of amblyopia Refractive error found by cycloplegic refraction requires full correction, but the only effective method of treating amblyopia is to occlude the non-amblyopiceye. In a very young child a dramatic improvement will occur with effective occlusion. Improvement in vision is usually very slow after the age of six years. is the most effective method of occlusion. The patch should be worn on the face so that it totally covers the better eye. If the amblyopia is not severe or has improved with patching, then less rigorous occlusion can be used such as covering of the spectacle lens of the better eye with a patch. This type of occlusion is useless in the case of marked amblyopia as the child will simply look over the top of the spectacles. When the vision is almost equal in both eyes, the spectacle lens can be occluded with a semi-transparent material. Atropine drops or ointment may be instilled into the non-amblyopic eye to blur the vision of that eye especially for close work and encourage the use of the amblyopic eye. However in most cases atropine is only partially effective. Occlusion is essential to improve most cases of amblyopia, but its use requires experience. The younger the child the faster the amblyopia will be improved by patching. This improvement can often be associated with a marked fall in vision of the originally better eye as the occlusion of that eye is producing deprivation amblyopia. Children who are patched must therefore be seen extremely frequently, especially when very young, to assess the progress of the amblyopic eye and of the occluded eye. Diplopia can occur if the vision of the amblyopic eye is improved. This can become a problem in children over seven when they are unable to fuse the image due to the absence of any binocular vision and sometimes cannot learn to suppress the second image.
- 14. Ophthalmology | Esotropian squint 14 Correction of the angle of squint Convergent squints which are the direct result of uncorrected hypermetropia may be completely corrected by prescribing the full hypermetropic correction as discovered by retinoscopy. Effective treatment of the amblyopic eye by occlusion is also necessary. The fully accommodative squint may well be cured in this way. If the spectacles fail to correct the squint and vision is practically equal in both eyes following occlusion, then consideration must be given to surgery. Care must be taken to assess whether one is treating a squint in which a binocular result can be expected or one which is solely a cosmetic problem. The potentially binocular squint is usually of recent onset and occurs in a child of two years of age and over in whom it can be inferred that binocular vision has developed to some extent. Orthoptic assessment should show the presence or absence of binocular vision. The potentially binocular squint should be operated on as soon as possible if it persists after the refractive error has been corrected and occlusion has achieved equal vision in both eyes or has failed to produce further improvement in the squinting eye. If possible the child should be able to alternate, i.e. use either eye for fixation. This situation is ideal but is not always achieved. The child with a squint who does not show any potential binocular vision should only be operated on to achieve an acceptable cosmetic result, but the visual acuity of each eye should be tested at intervals and further occlusion used if necessary. It is not advisable to operate on a squint in a child under seven years of age until a reasonable attempt has been made to overcome any amblyopia. Children with a fully accommodative squint should not have an operation with the intention of reducing the strength of their spectacle correction because as the child becomes older his accommodative ability decreases and he will need to have his hypermetropia corrected in order to see clearly. This will then tend to cause divergence as the cause of the squint was uncorrected hypermetropia. Thus the treatment is the correction of the hypermetropia and not surgical interference with a normal physiological reflex.
- 15. Ophthalmology | Esotropian squint 15 In children with a low hypermetropic correction who have binocular vision it is nevertheless reasonable to consider a short trial of orthoptic training to improve binocularity in an attempt to control the squint without spectacles.
- 16. Ophthalmology | Esotropian squint 16 References:- 1- A text book of clinical ophthalmology 3rd edition by Ronald Pitts Crick FRCS, FRCOphth Honorary Consultant Ophthalmologist, King's College Hospital, London. And Peng Tee Khaw PhD, FRCP, FRCS, FRCOphth, FIBiol, FRCPath, FMedSci Professor of Glaucoma and Wound Healing Consultant Ophthalmic Surgeon, Director, Wound Healing Research Unit Moorfields Eye Hospital and Institute of Ophthalmology, University College, London. 2- Wills Eye Hospital Atlas of Clinical Ophthalmology , The, 2nd Edition. 3- American Academy of ophthalmology. 4- Ophthalmology lecture of MUCOM by Dr. Hasanain Shbir. 5- Web reference in terms of images.