
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Hyphema
Similar to Hyphema (20)
More from Ali Faris
More from Ali Faris (20)
Recently uploaded
Recently uploaded (20)
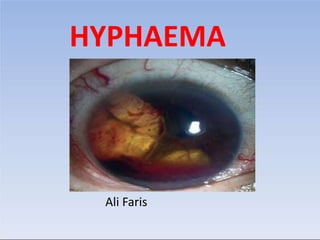
Hyphema
- 2. Definition: Blood in the anterior chamber of eye is called Hyphema.
- 3. Pathophysiology: • Compressive force to the globe or trauma can result in injury to the iris, ciliary body, trabecular meshwork, and their associated vasculature. The shearing forces from the injury can tear these vessels and result in the accumulation of blood cells within the anterior chamber. Fig; Bleeding from the ciliary body
- 4. Classification Etiological: 1. Traumatic hyphaema - most commonly blunt trauma 2. Strenuous conditions - Whooping cough, Asthma etc. 3. Blood dyscrasia -Aplastic anaemia, leukemia, hemophilia, von Willebrand disease etc. 4. Neovascularization (Rubeosis iridis) - Diabetes mellitus
- 5. Classification Etiological: 5. Miscellaneous -Intraocular tumors (retinoblastoma, iris melanoma etc.) - Vascular anomaly - juvenile xanthogranuloma (JXG) - Secondary to ocular surgery or laser -Medications with anticoagulant properties (aspirin, NSAIDs, warfarin or clopidogrel etc.)
- 6. Classification Clinical: 1. Mild or simple hyphema (2-3mm) 2. Moderate hyphema (3-5mm) 3. Severe hyphema – more than half of A/C 4. Total hyphema – A/C full of blood
- 7. Grading Hyphaemas can be graded from I-IV in the following manner:
- 8. ????
- 9. Presentation
- 10. secondary hemorrhage with raised IOP and increased risk of glaucoma Hyphaema: Small with low risk of raised IOP
- 11. Presentation • Symptoms: Symptoms can be variable depending on the etiology. Typically patients complain of blurry vision, pain, headahce, photophobia, H/O trauma. • Signs: Blood or clot or both in the AC, usually visible without a slit lamp.
- 12. Examinations/Work-up 1. History: Detailed including - - Mechanism of injury - Time of injury with time of visual loss(if any) - H/O medications (aspirin, warfarin etc.) - H/O Sickle cell disease (familial or personal?) -Any H/O coagulopathy- bleeding gums, epistaxis etc.
- 13. Examinations/Work-up 2. Ocular examinations: -Rule out any rupture globe or penetrating injuries - Visual acuity - IOP - Slit lamp examination - B-scan (gently) if A/C filled with blood -CT may be done if suspected orbital fracture
- 14. Management
- 15. Treatment: General 1. coagulation abnormality should be excluded. 2. anticoagulant medication should be discontinued 3.NSAIDs should not be used for analgesia. 4.specialist advice 5.Hospital admission 6.limiting activity 7.protective eye shield.
- 16. Treatment: Medical • Topical prostaglandins, beta-blockers and/or a topical • Miotics should also be avoided • Topical steroids • Atropine with a large hyphaema • Antifibrinolysis
- 17. Treatment: Surgical Laser photocoagulation of angle bleeding points via a gonioprism, though gonioscopy should probably be deferred for 5–6 days post- injury.
- 18. Anterior chamber paracentesis or surgical evacuation of blood • required in 5% • Indications for surgery include: 1. total hyphaema, 2. an IOP of >50 mmHg for 2 days or an IOP >35 mmHg for 5 days. • reduces the risk of permanent corneal staining and optic atrophy and prevents the occult development of peripheral anterior synechiae and chronic secondary glaucoma
- 20. THANK YOU
Editor's Notes
- Grade 0: No visible layering, but red blood cells within the anterior chamber (microhyphaema) Grade I: Layered blood occupying less than 1/3 of the anterior chamber Grade II: Blood filling 1/3 to 1/2 of the anterior chamber Grade III: Layered blood filling ½ to less than total of the anterior chamber Grade IV: Total clotted blood, often referred to as blackball or 8-ball hyphaema
- Traumatic hyphaema. (A) Small hyphaema; (B)total hyphaema; (C) corneal blood staining due to sustained high intraocular pressure associated with a total hyphaema Corneal blood staining (CBS) is a complication of hyphema and increased intraocular pressure (IOP). Spontaneous clearing can take up to 3 years, starting at the periphery.1 Factors that increase the risk of CBS include total hyphema, rebleeding, and endothelial dysfunction.2 Management options for hyphema with increased IOP include trabeculectomy, anterior chamber washout, and pharmacotherapy with topical steroids and cycloplegics.
- A coagulation abnormality, particularly a haemoglobinopathy, should be excluded. Any current anticoagulant medication should be discontinued after liaison with a general physician to assess the risk. NSAIDs should not be used for analgesia. Likewise, specialist advice should be sought regarding the management of a patient with a haemoglobinopathy, particularly before administering high-risk medication . Hospital admission may be required for a large hyphaema. Strict bed rest is probably unnecessary, but substantially limiting activity is prudent and the patient should remain in a sitting or semi-upright posture, including during sleep. A protective eye shield should be worn.
- ○ Topical prostaglandins, beta-blockers and/or a topical or systemic CAI is administered, depending on the IOP. CAI should not be used in sickle haemoglobinopathies.Miotics should also be avoided as they may increase pupillary block and disrupt the blood–aqueous barrier. ○ Occasionally a hyperosmotic agent is needed, though as with CAI and alpha-agonists a high threshold is adopted in sickle patients. ○ Topical steroids should be used since they reduce the risk of secondary haemorrhage and suppress inflammation. ○ Atropine is often recommended in patients with a large hyphaema to achieve constant mydriasis and to reduce the chance of secondary haemorrhage. ○ Antifibrinolysis with systemic aminocaproic acid (ACA) or tranexamic acid may be considered under higher-risk circumstances such as recurrent bleeding.
- • is required in around 5%. Indications for surgery include a total hyphaema, an IOP of >50 mmHg for 2 days or an IOP >35 mmHg for 5 days. Surgical intervention reduces the risk of permanent corneal staining and optic atrophy and prevents the occult development of peripheral anterior synechiae and chronic secondary glaucoma. Particular vigilance is required in patients with sickle-cell anaemia (even moderate pressure elevation can lead to optic atrophy), patients with prior glaucomatous optic neuropathy and in young children with a risk of amblyopia. A glaucoma filtration procedure may be necessary in some cases.