This document provides an overview of Class II malocclusions, including:
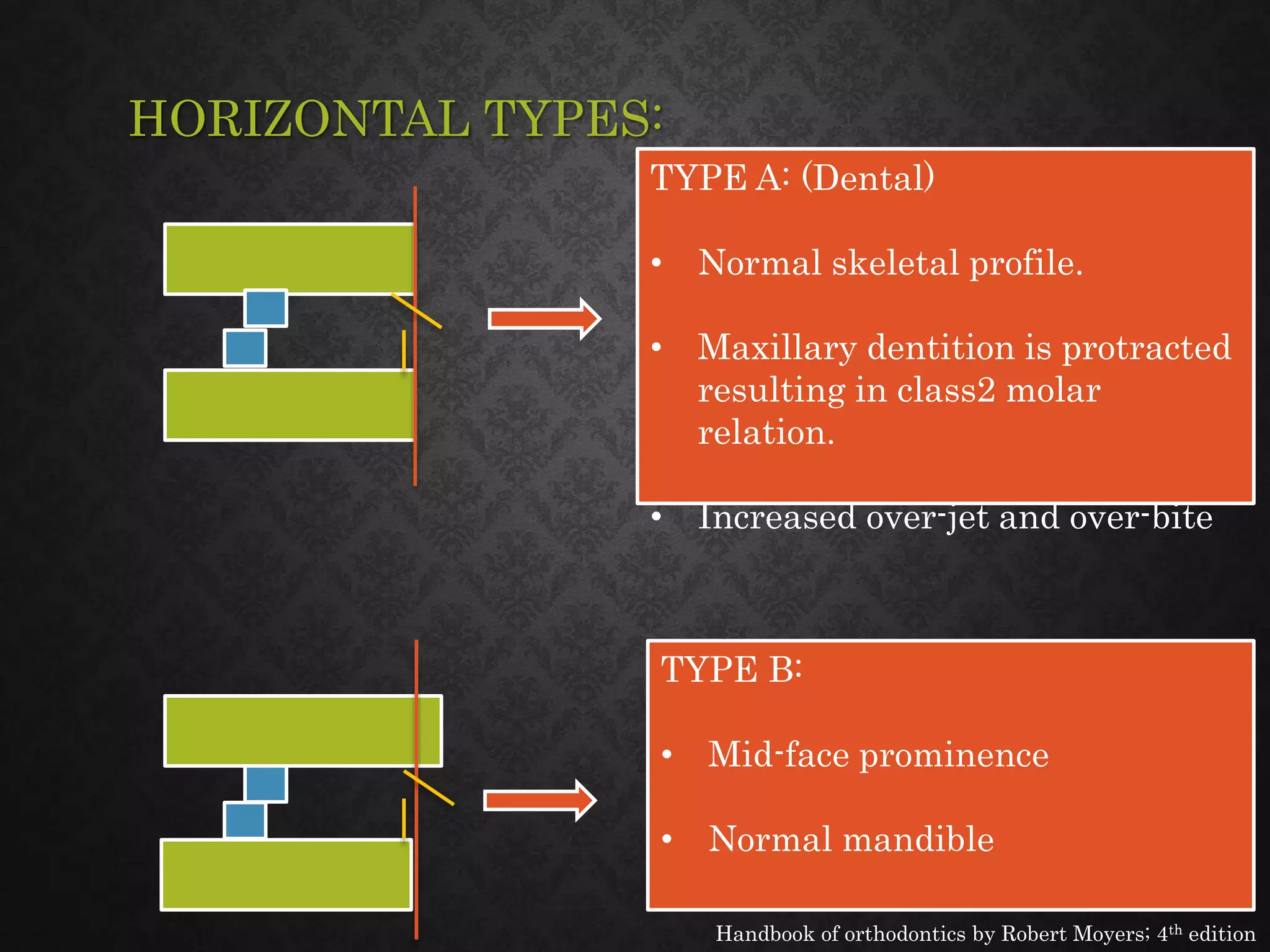
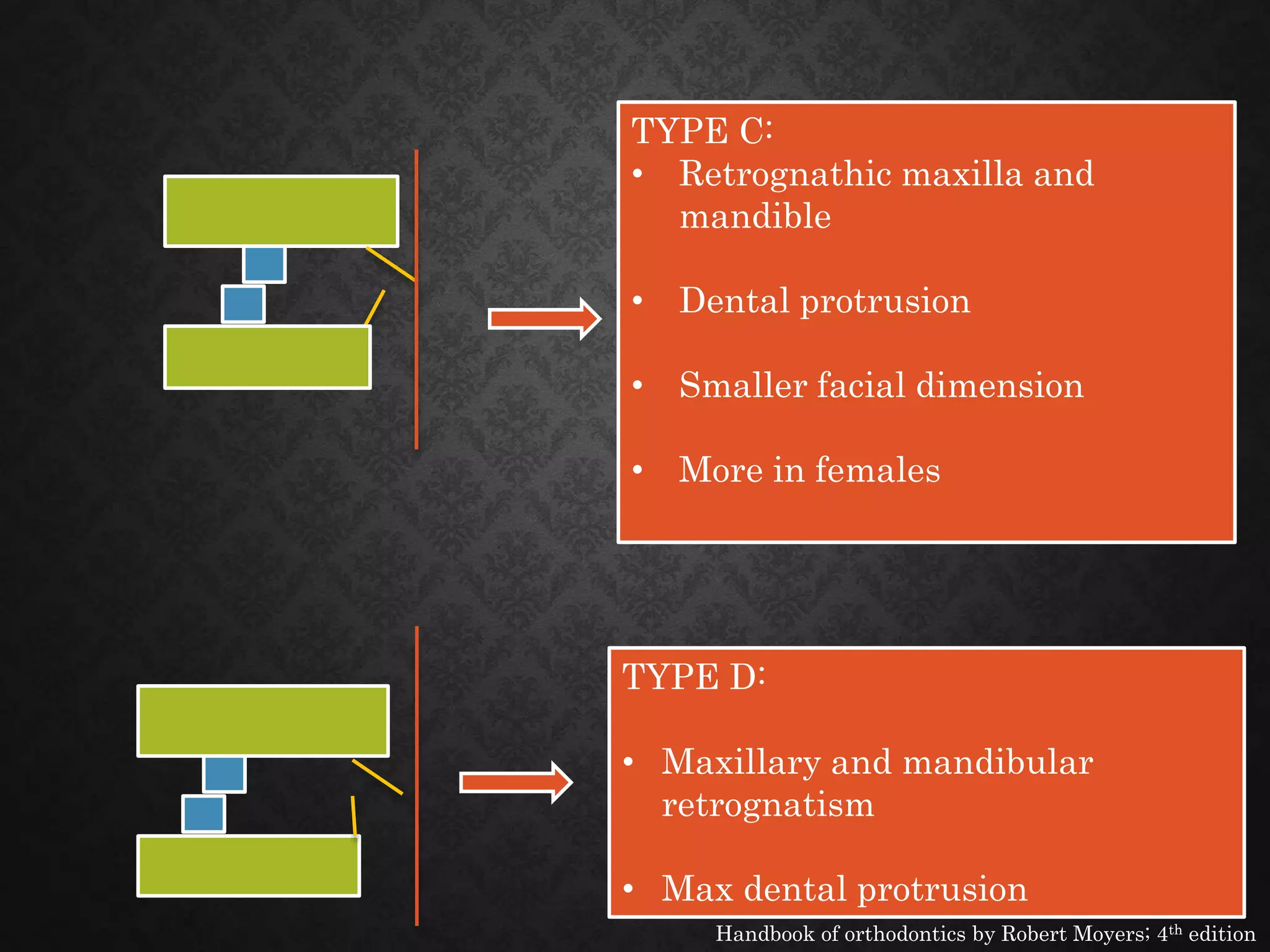
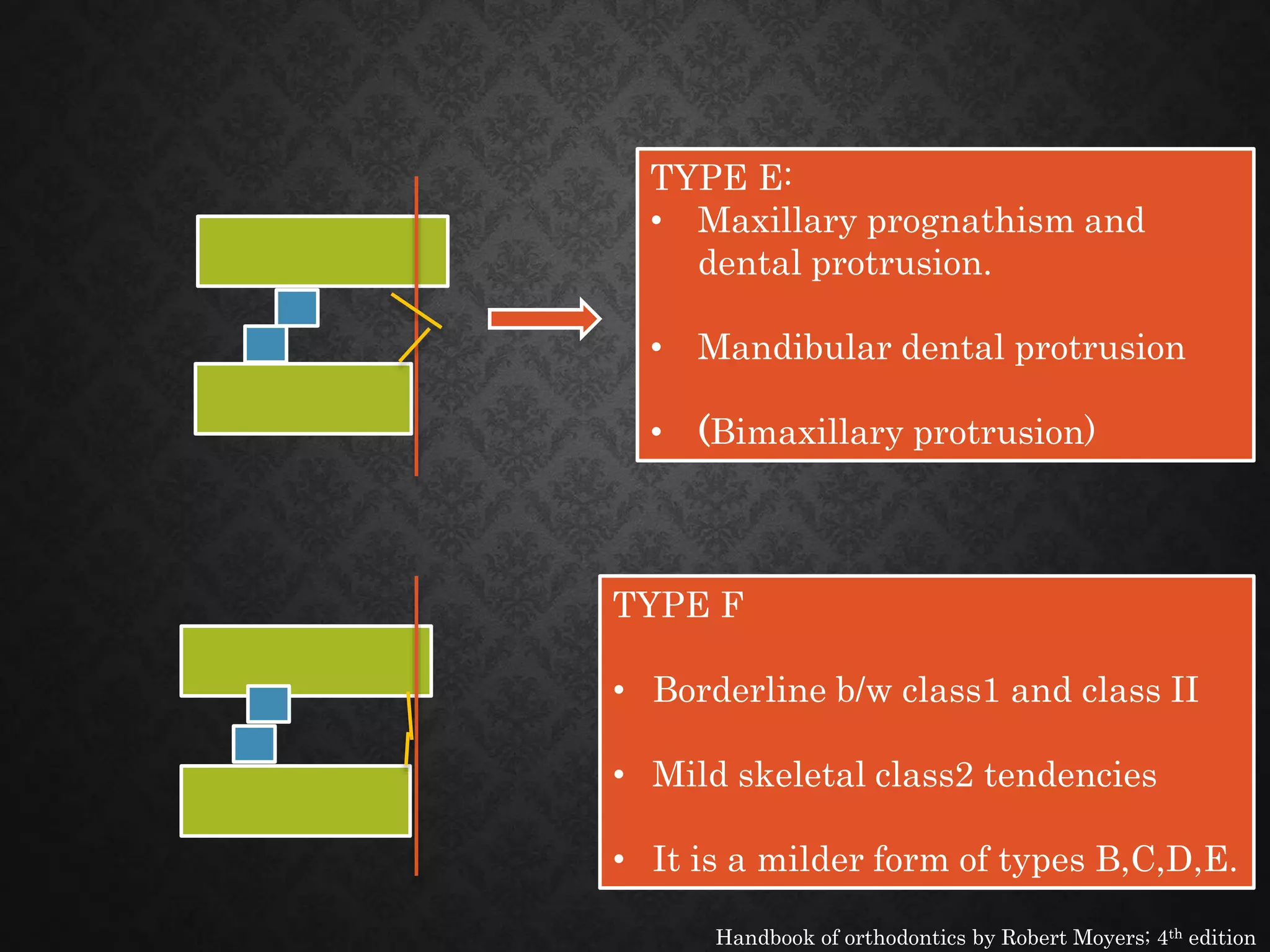
- Classification systems for Class II malocclusions described by Angle and Moyers.
- Common etiological factors like heredity and habits.
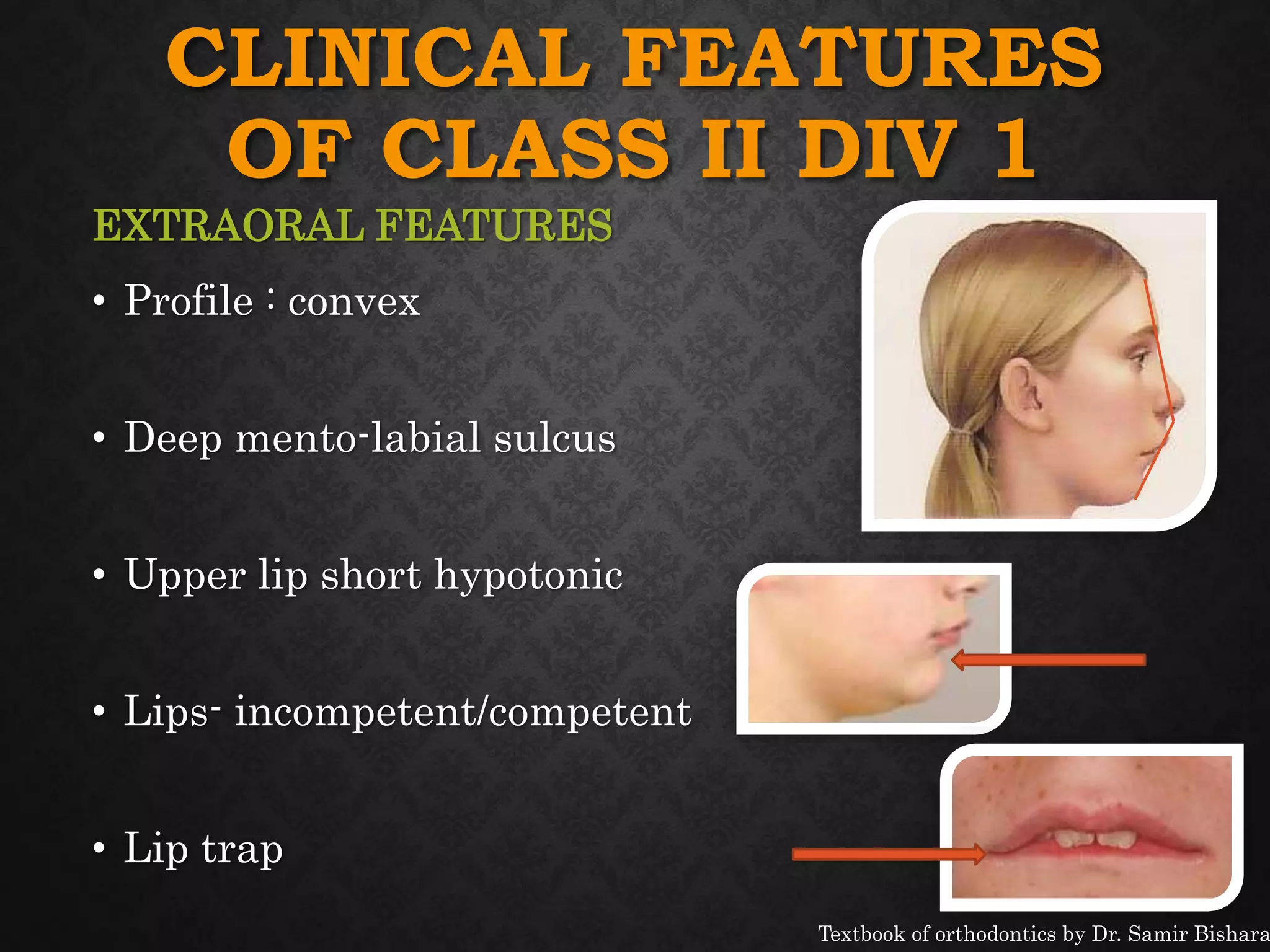
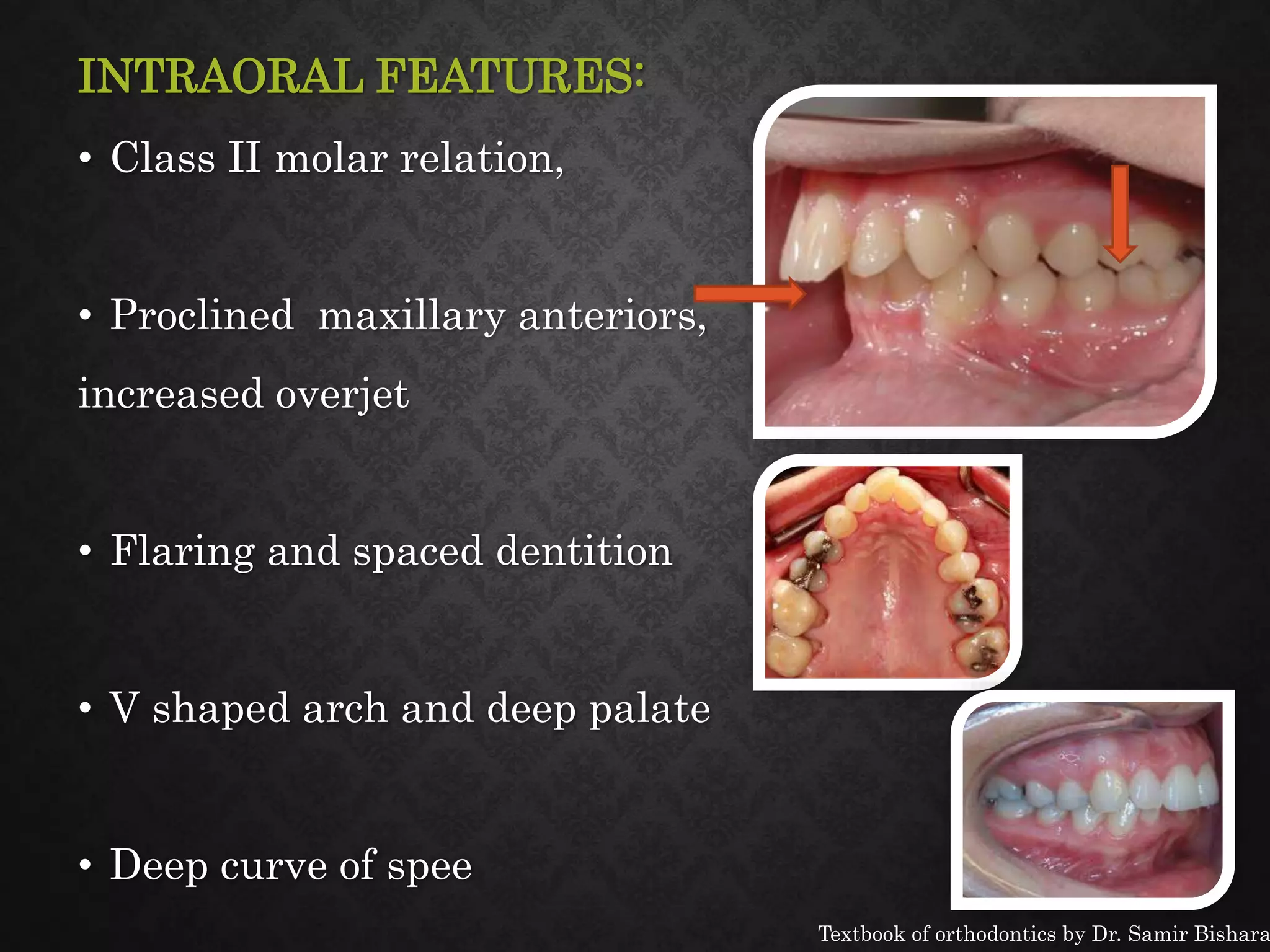
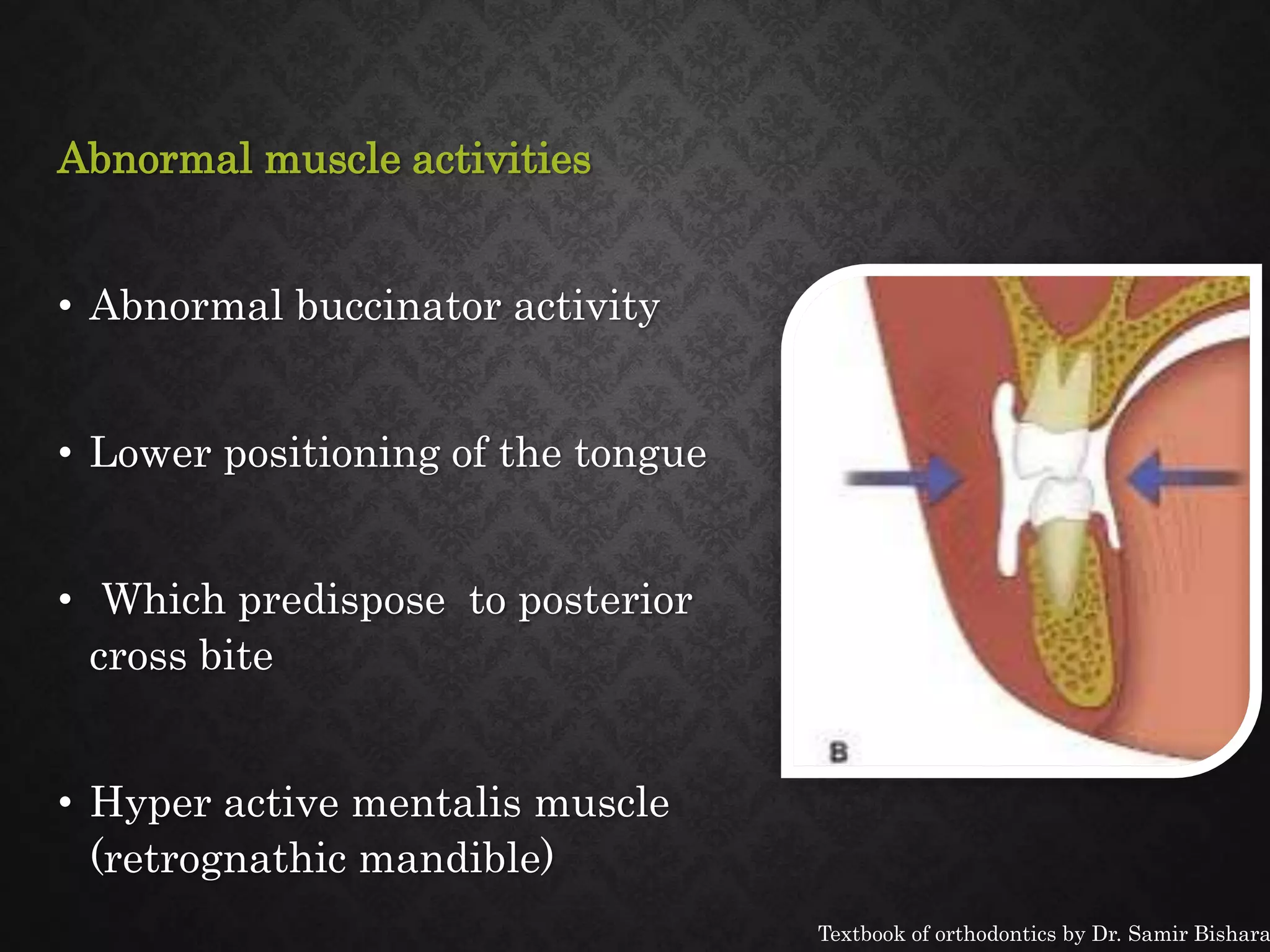
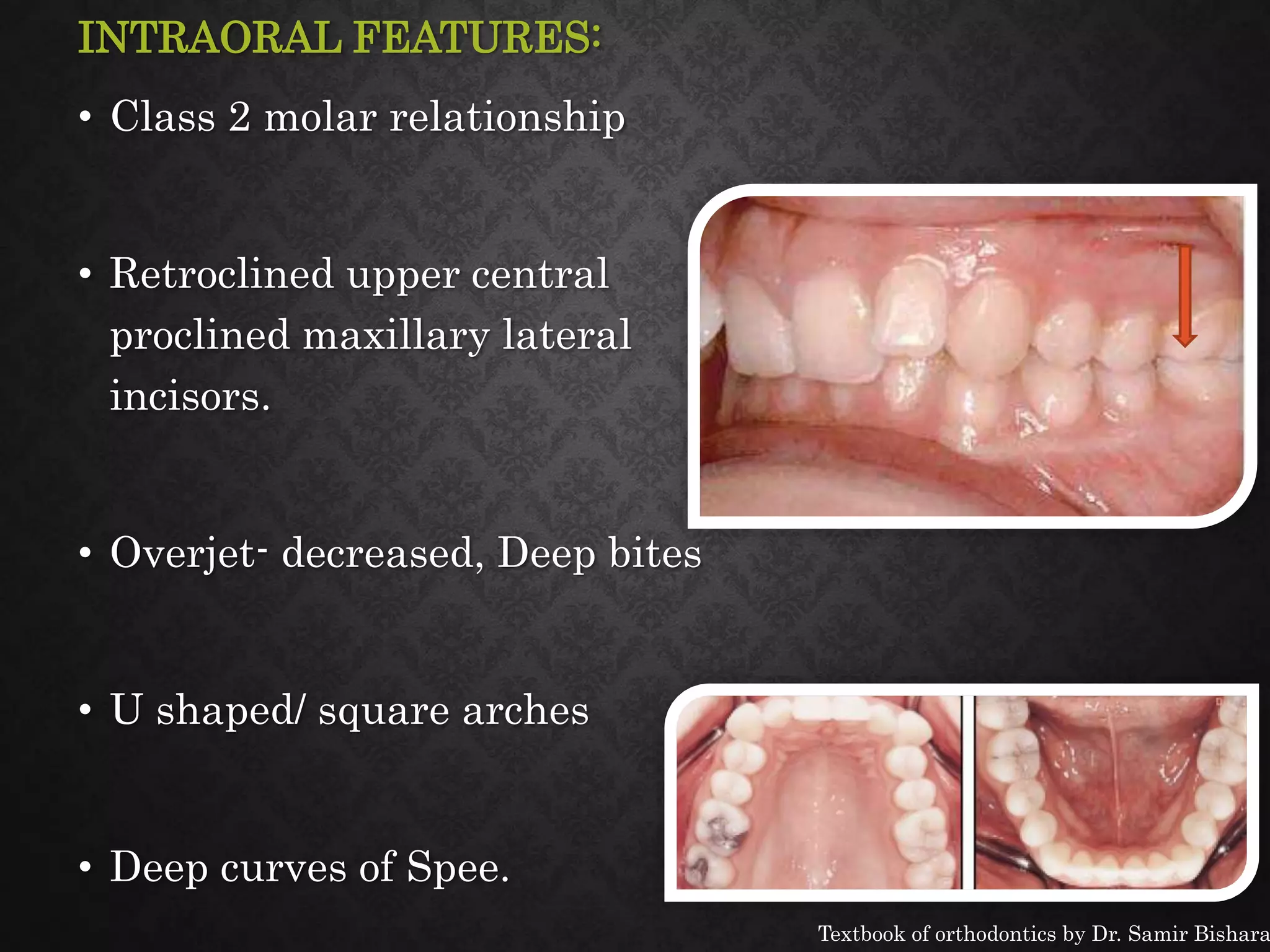
- Clinical features both intraorally and extraorally.
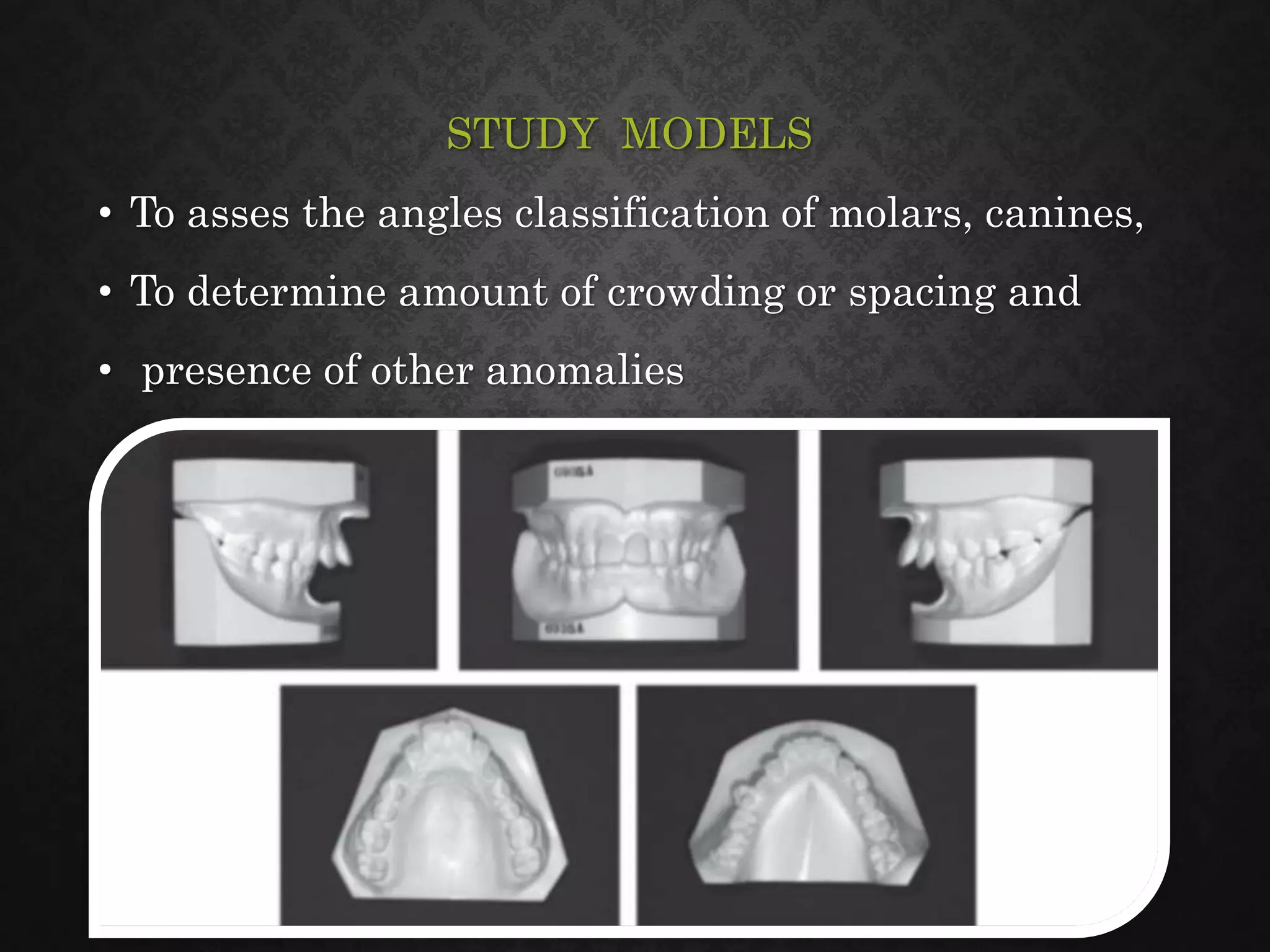
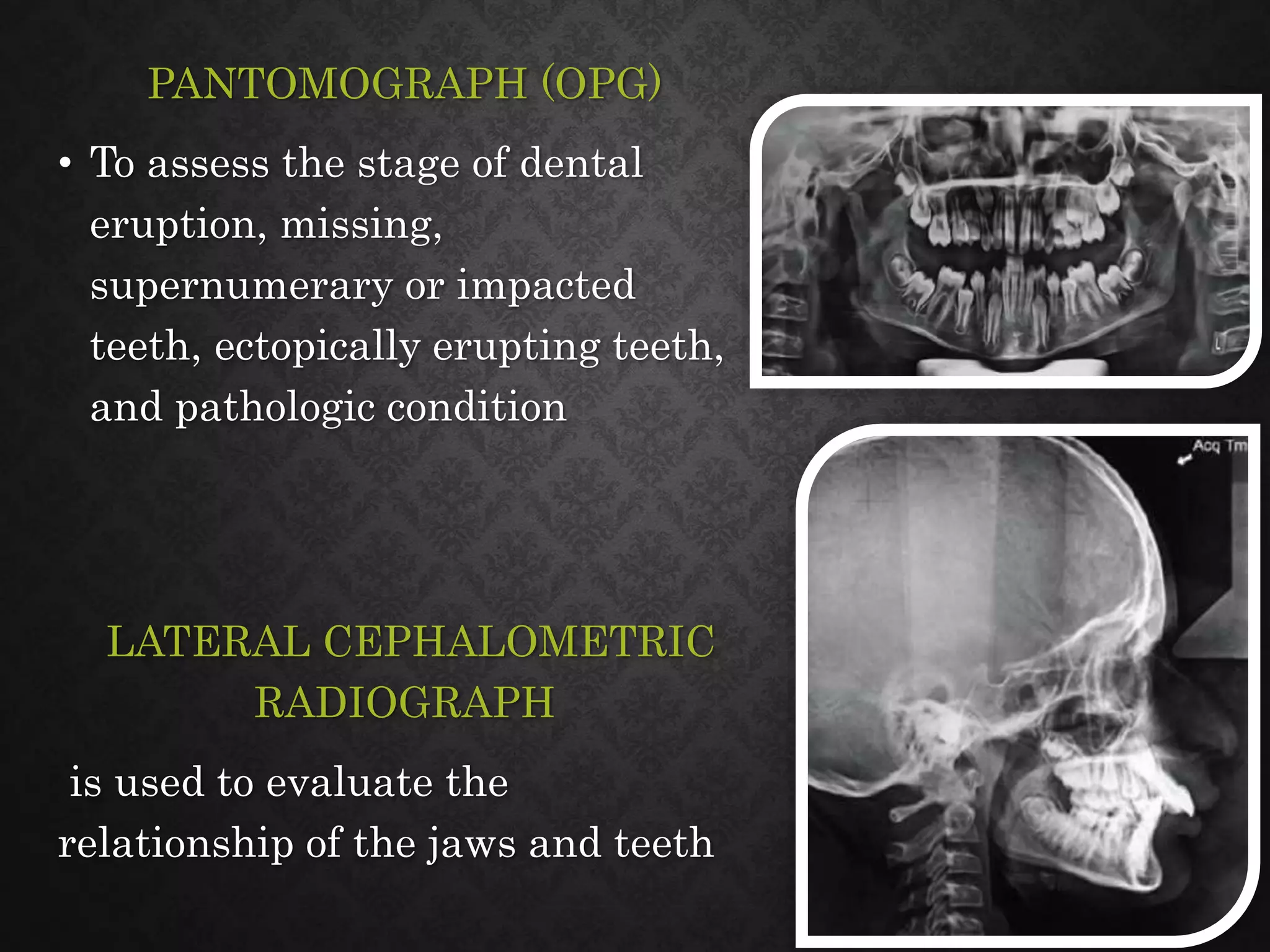
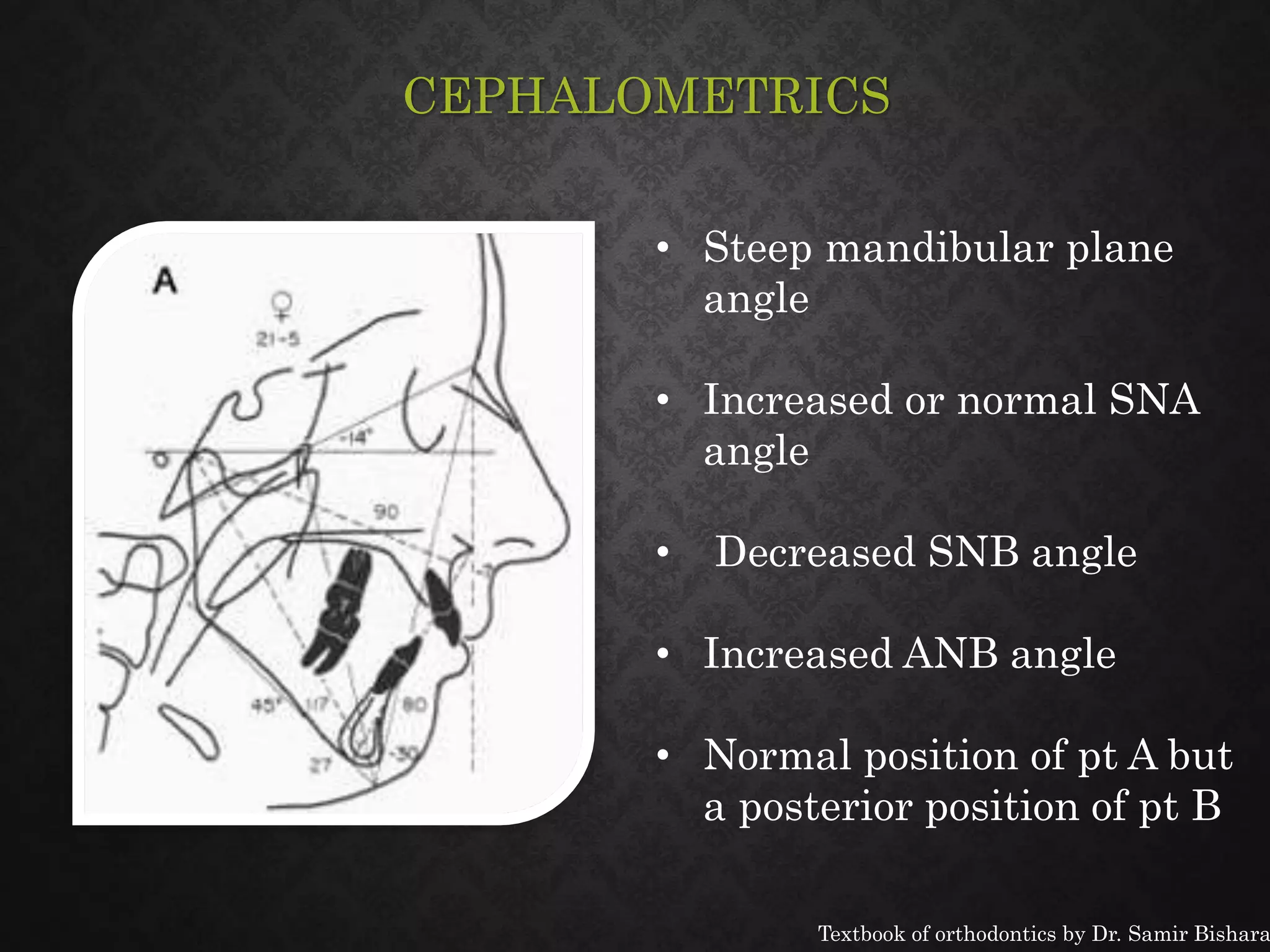
- Diagnostic tools and assessments including study models, photographs, and cephalometrics.
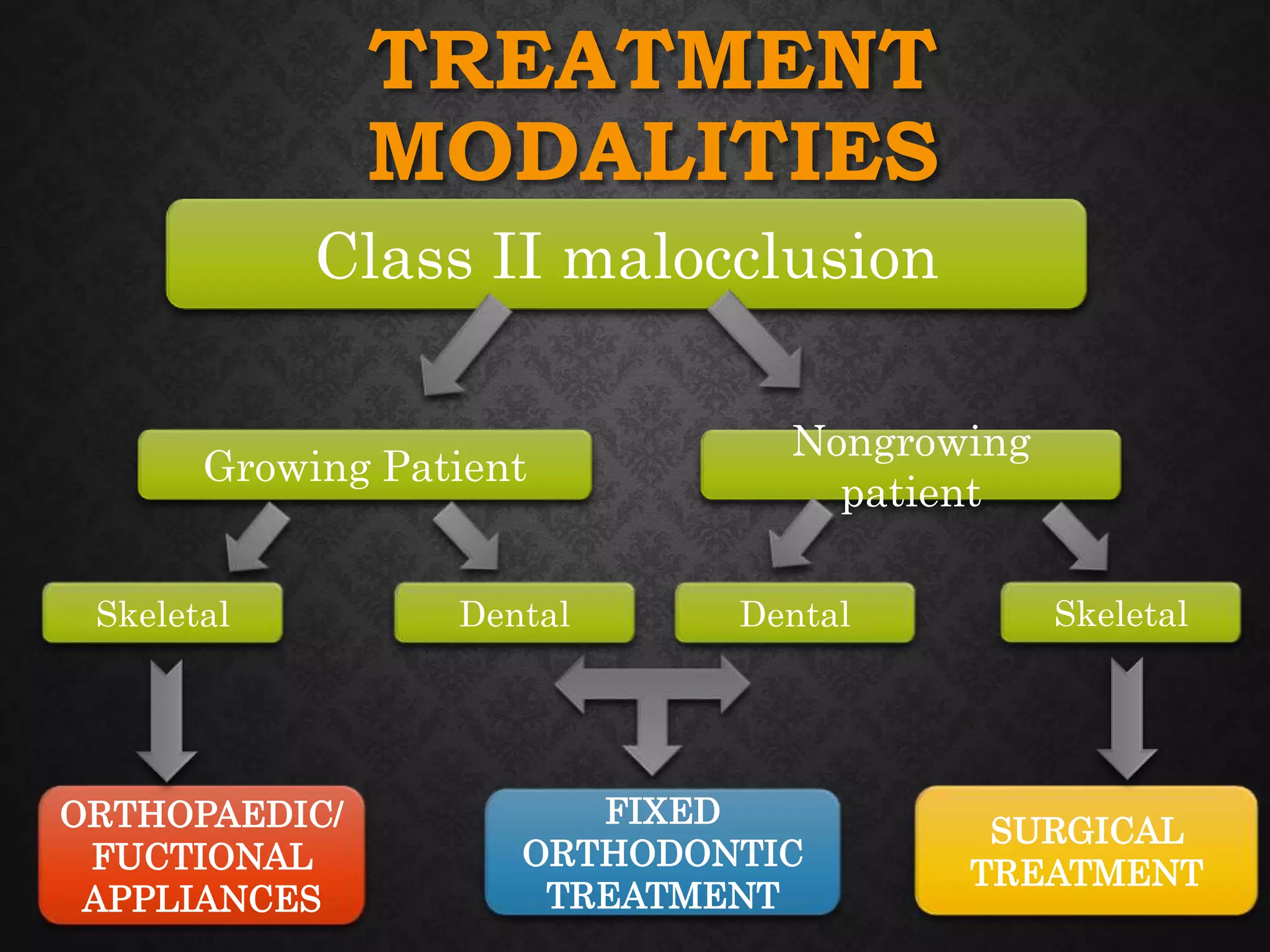
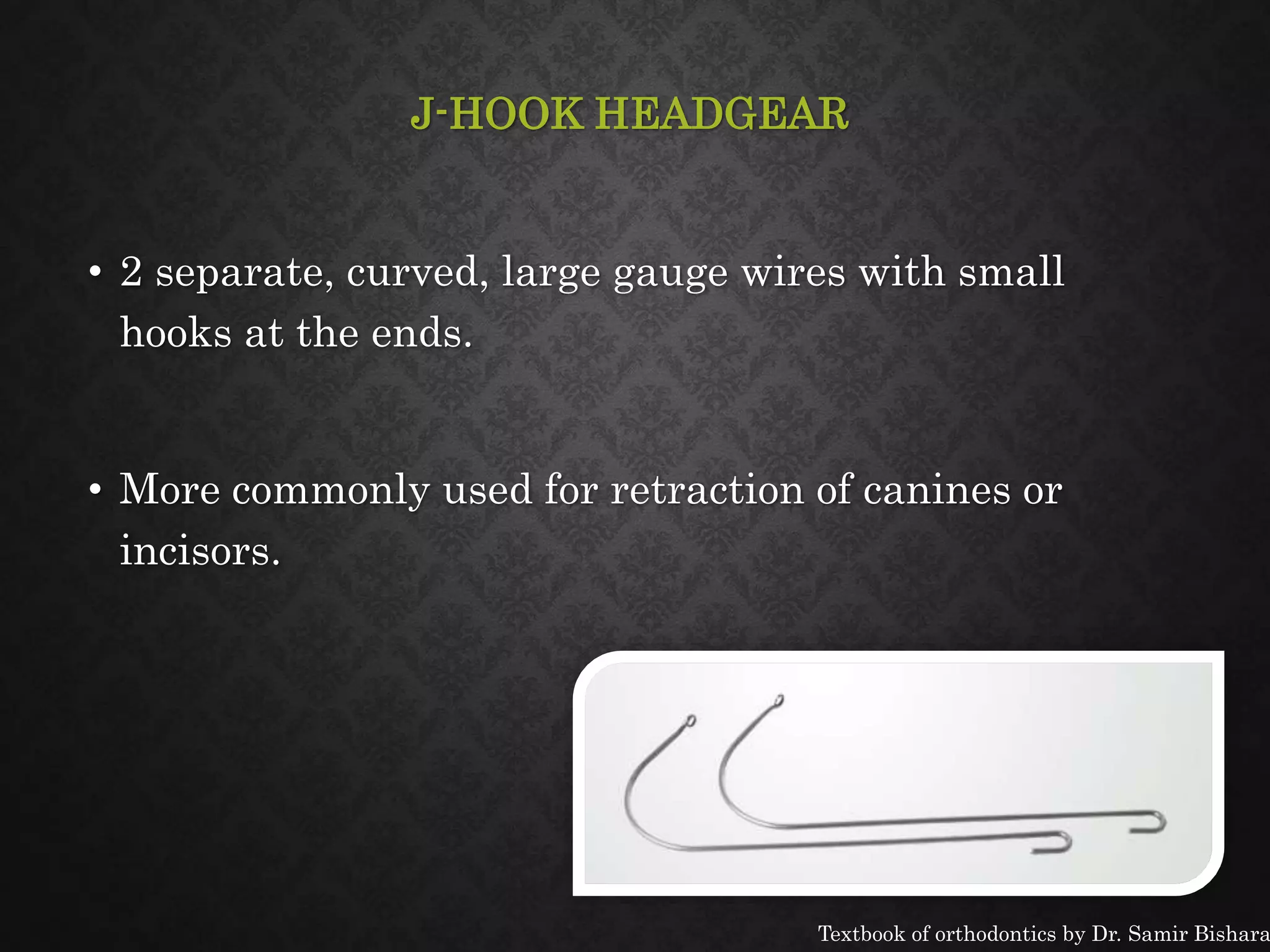
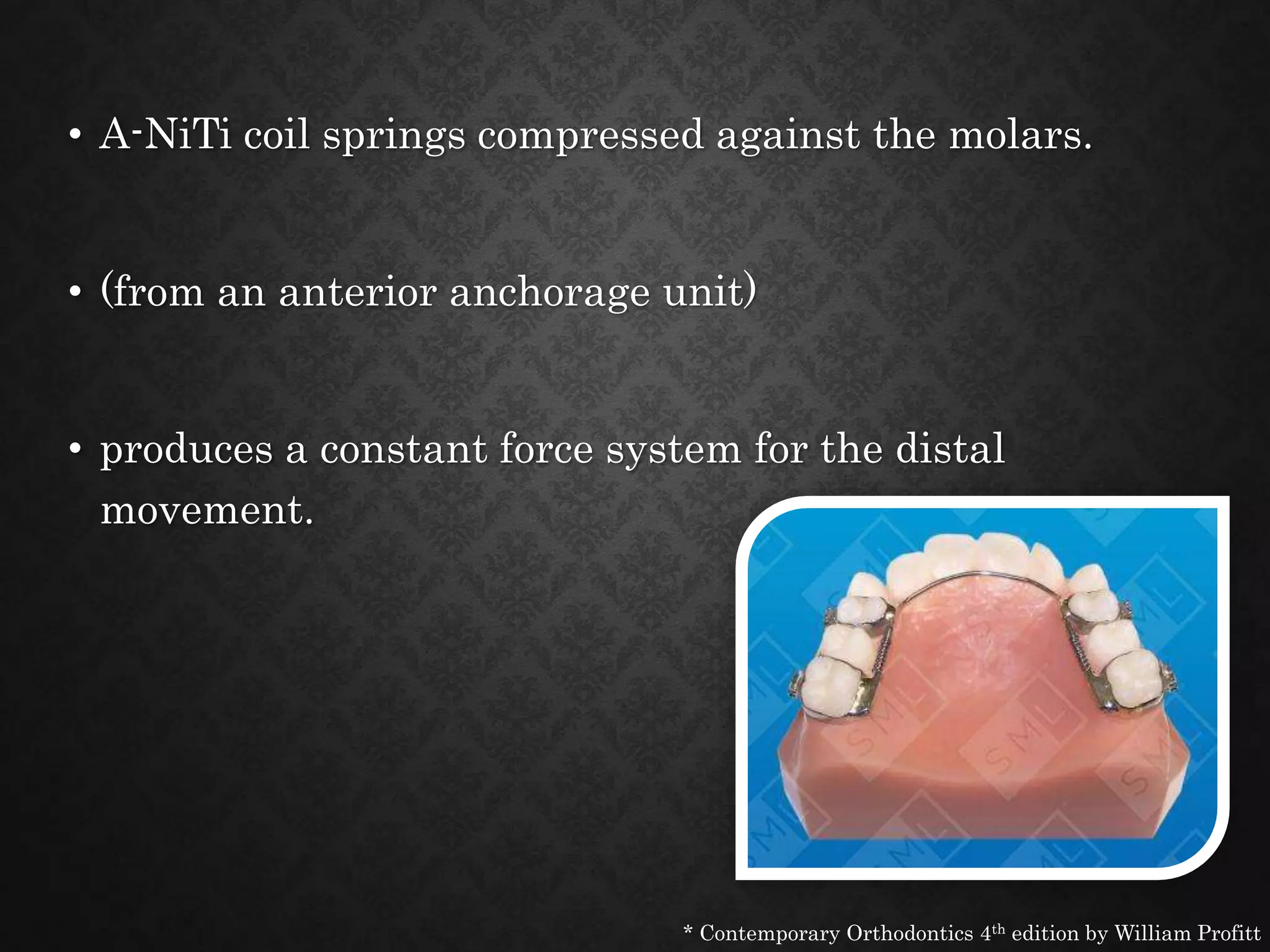
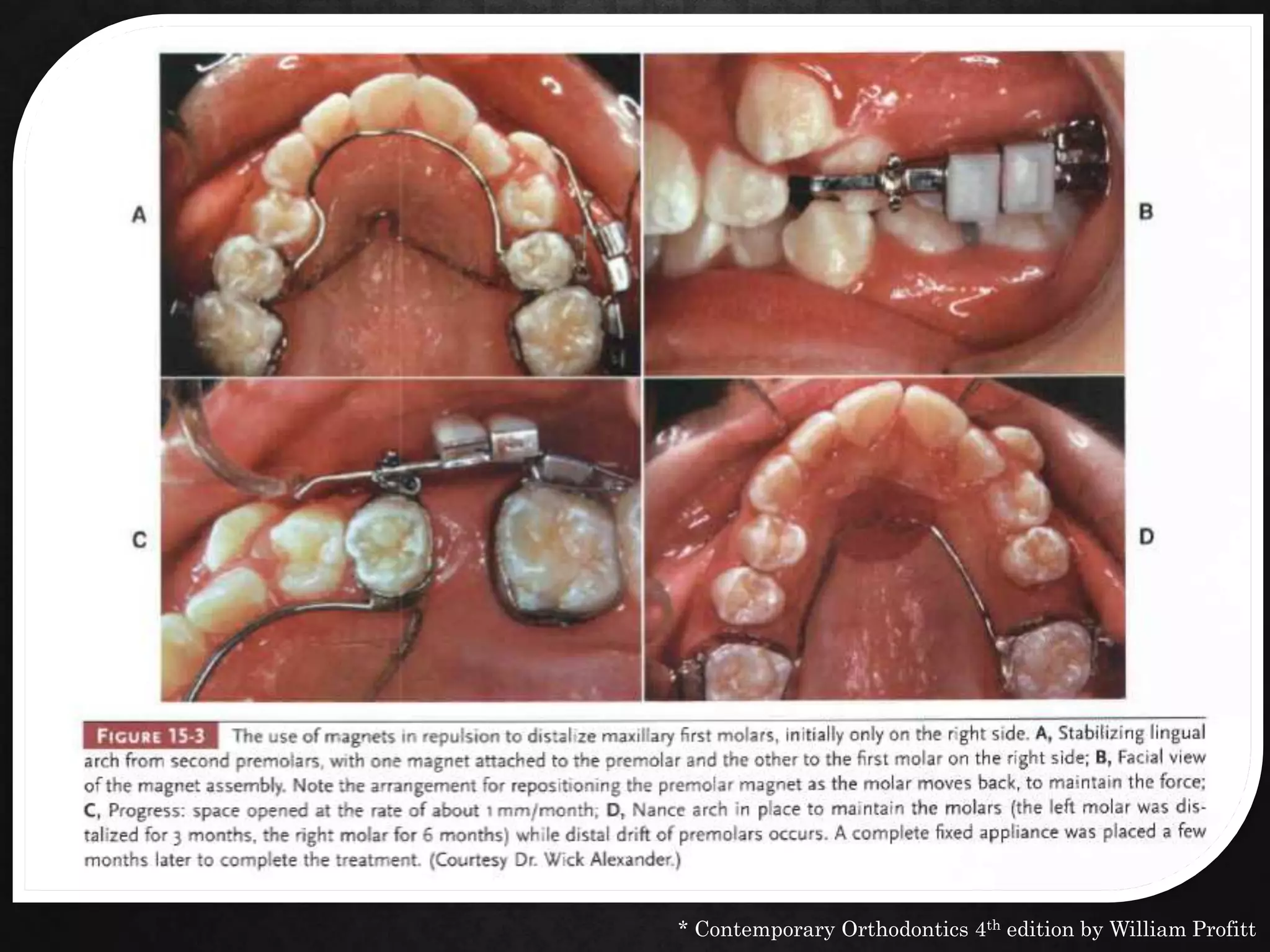
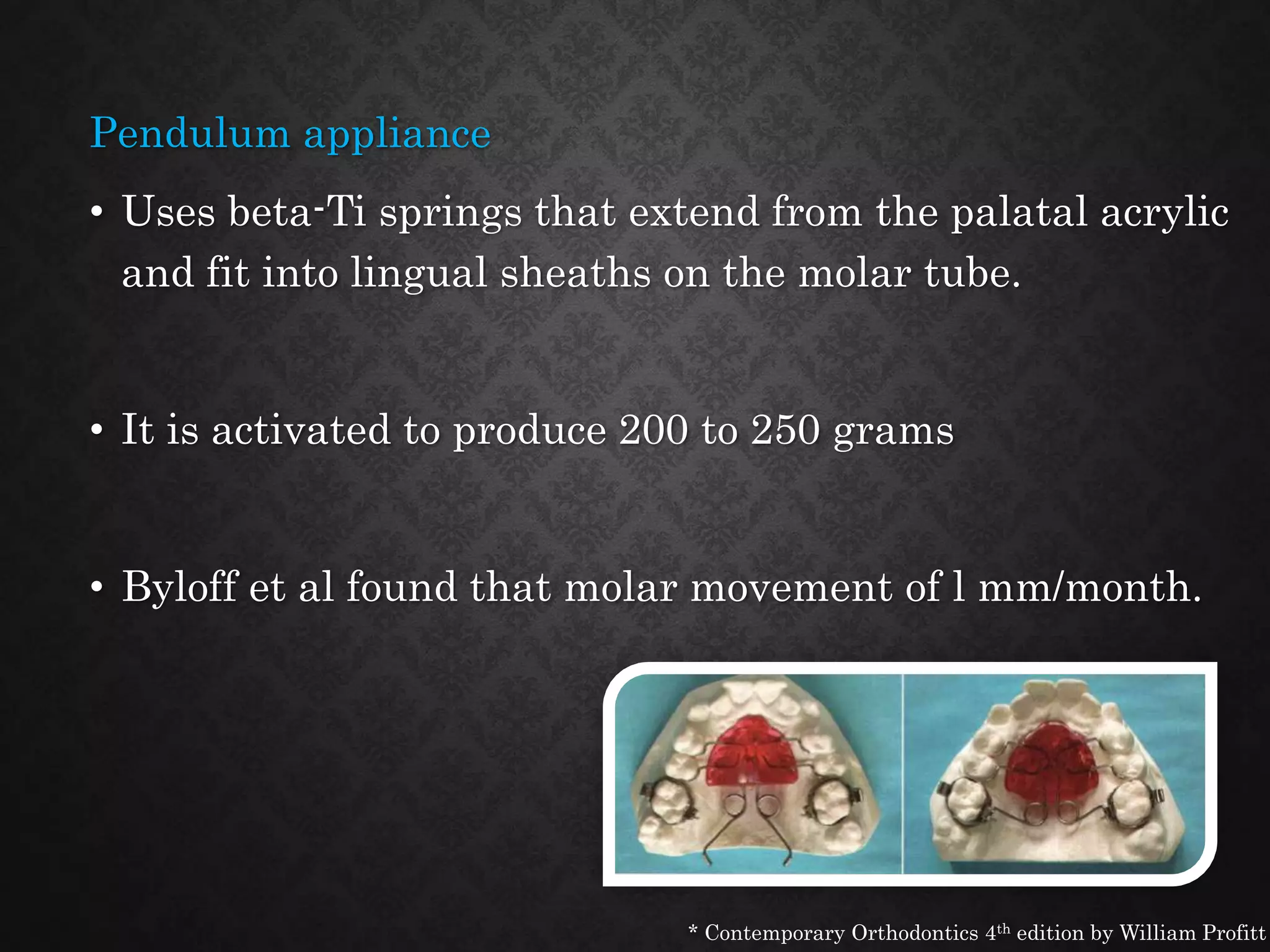
- Treatment modalities for Class II malocclusions in growing and non-growing patients, including functional appliances, headgear, fixed appliances, and orthognathic surgery.




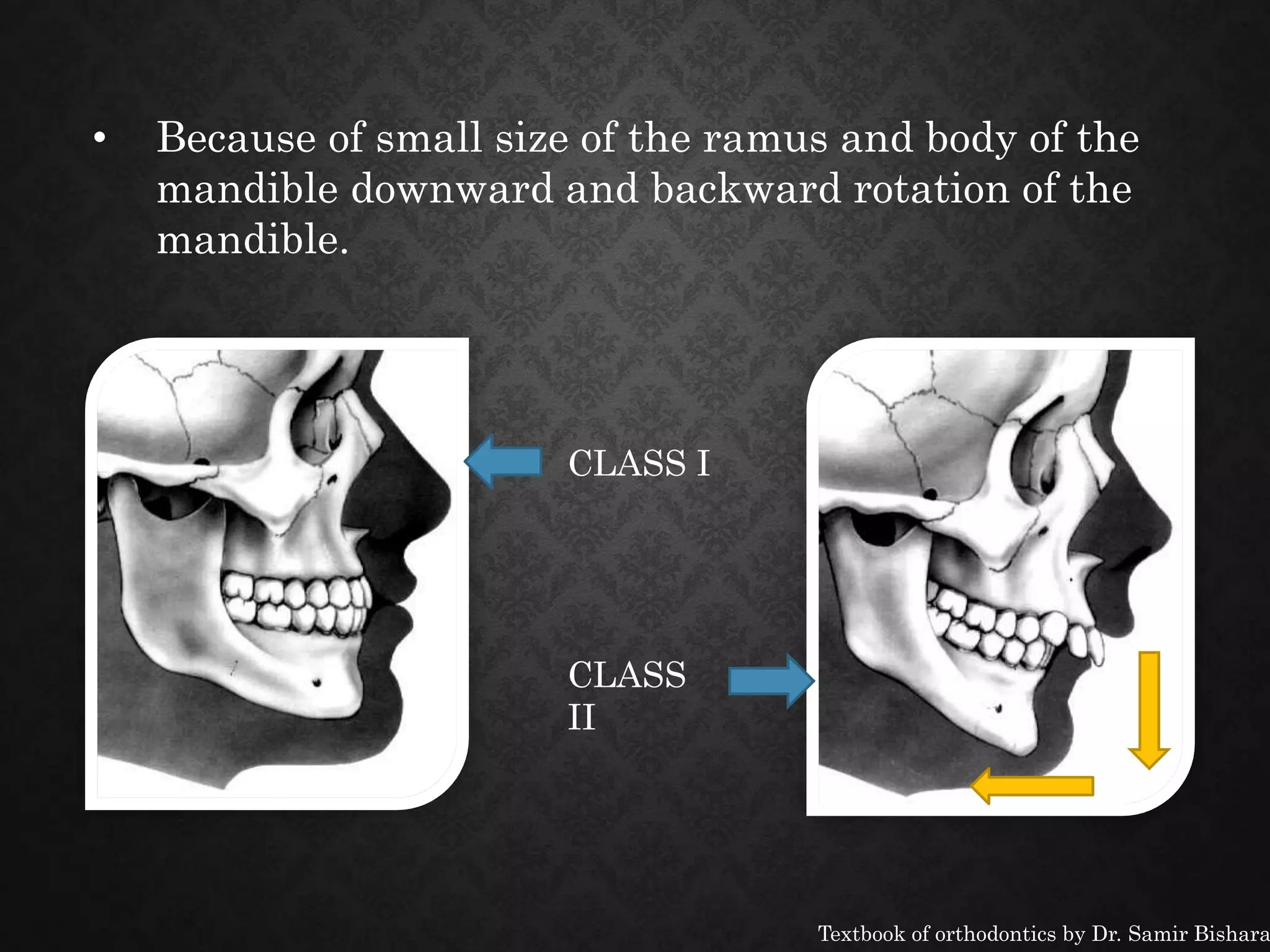
![SKELETAL CLASS II
MALOCCLUSIONS
• Skeletal discrepancies are often associated with
dental Class II malocclusions.
A] Mandibular Deficiency
B] Maxillary Excess
Textbook of orthodontics by Dr. Samir Bishara](https://image.slidesharecdn.com/classiimalocclusion-161213170920/75/Class-ii-malocclusion-10-2048.jpg)