Lumbar Puncture
•
19 likes•10,659 views

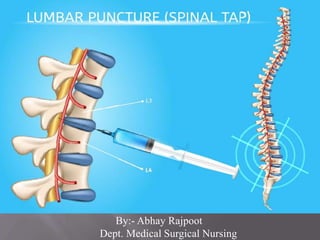
A lumbar puncture (spinal tap) is performed in your lower back, in the lumbar region. During a lumbar puncture, a needle is inserted between two lumbar bones (vertebrae) to remove a sample of cerebro-spinal fluid. This is the fluid that surrounds your brain and spinal cord to protect them from injury.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Lumbar Puncture
Similar to Lumbar Puncture (20)
More from Abhay Rajpoot
More from Abhay Rajpoot (20)
Recently uploaded
Recently uploaded (20)
Lumbar Puncture
- 1. By:- Abhay Rajpoot Dept. Medical Surgical Nursing
- 2. The cervical area consists of seven vertebrae in the neck. TThe spinal column is made up of 33 vertebrae that are separated by spongy disks and classified into distinct areas: he thoracic area consists of 12 vertebrae in the chest area. The lumbar area consists of five vertebrae in the lower back area. The sacrum has five, small fused vertebrae. The four coccygeal vertebrae fuse to form one bone, called the coccyx or tailbone. The spinal cord, a major part of the central nervous system, is located in the vertebral canal and reaches from the base of the skull to the upper part of the lower back. The bones of the spine and a sac containing cerebrospinal fluid surround it. The spinal cord carries sense and movement signals to and from the brain and controls many reflexes.
- 4. Lumbar puncture (spinal tap) is performed in your lower back, in the lumbar region. During lumbar puncture, a needle is inserted between two lumbar bones (vertebrae) to remove a sample of cerebrospinal fluid — the fluid that surrounds your brain and spinal cord to protect them from injury. A lumbar puncture can help diagnose serious infections, such as meningitis; other disorders of the central nervous system, such as Guillain-Barre syndrome and multiple sclerosis; or cancers of the brain or spinal cord. Sometimes doctors use lumbar puncture to inject anesthetic medications or chemotherapy drugs into the cerebrospinal fluid.
- 5. 1. Lumbar puncture may be done to: Collect cerebrospinal fluid for laboratory analysis Measure the pressure of your cerebrospinal fluid Inject spinal anesthetics, chemotherapy drugs or other medications Inject dye (myelography) or radioactive substances into cerebrospinal fluid to make diagnostic images of the fluid's flow 2.To obtain CSF for the diagnosis of: Meningitis Meningoencephalitis Subarachnoid hemorrhage Malignancy – diagnosis and treatment
- 6. Serious bacterial, fungal and viral infections, including meningitis, encephalitis and syphilis Bleeding around the brain (subarachnoid hemorrhage) Certain cancers involving the brain or spinal cord Certain inflammatory conditions of the nervous system, such as multiple sclerosis and Guillain-Barre syndrome.
- 7. Unstable patient with cardiovascular or respiratory instability Localized skin/soft tissue infection over puncture site Evidence of unstable bleeding disorder Platelets < 50,000 or clotting factor deficiency Age >65 Reduced GCS Recent history of seizure Focal neurological signs Abnormal respiratory pattern Hypertension with bradycardia and deteriorating consciousness
- 8. Most CSF trays come with: Anesthetic such as: Topical - Zylocaine cream Lidocaine 1% with 25 gauge needle and syringe Provide-iodine solution Drapes, gauze, and bandages Manometer Spinal needle, usually 22 gauge 1.5 in for < 1 yr 2.5 in for 1 year to middle childhood 3.5 in for older children and adolescents Larger for large adolescents
- 10. Consent Explain procedure Vital sign Investigation Positioning Skin preparation Article preparation
- 11. Assess the general condition of the patient and check all the laboratory investigations.preapare all the articles Wash hands Wear the gloves and maintain sterile field Performed with the patient in the lateral recumbent position. Spinal needles entering the subarachnoid space at this point are well below the termination of the spinal cord. Apply topical anesthetic 30-45 min prior to procedure
- 12. Spinal cord ends at L1-L2, so sites for puncture are located at L3-L4 or L4-L5 Restrain patient in lateral decubitus position Maximally flex spine without compromising airway Keep alignment of feet, knees and hips Position head to left if right handed
- 15. Restrain infant in the seated position with maximal spinal flexion Hold infant’s hands between flexed legs with one hand and flex head with the other hand Drape patient below buttocks and fenestrated drape opening over puncture site Insert needle so bevel is parallel to spinal cord (Bevel left or right) Cannot measure pressure accurately in this position
- 16. Cleanse skin with povidone iodine from puncture site radially out to 10 cm and ALLOW TO DRY Drape below patient and around site with fenestrated drape Anesthetize with lidocaine if topical not used by: Intradermally raising a wheal at needle insertion site Advance needle through wheal to desired interspace
- 17. Careful not to inject into a blood vessel or spinal canal Insert spinal needle with stylet with bevel up to keep cutting edge parallel with nerve and ligament fibers Hold needle firmly A “pop” of sudden decrease in resistance indicates that ligamentum flavum and dura are punctured Remove stylet and check for flow of spinal fluid If no fluid, then: Rotate needle 90° Reinsert stylet and advance needle slowly checking frequently for CSF Jugular vein compression can increase CSF pressure in low flow situations
- 18. If bony resistance is felt immediately then you are not in the spinal interspace If bony resistance is felt deeply, then withdraw needle to the skin surface and redirect more cephalad and increase patient flexion If bloody fluid that does not clear or that clots results, then withdraw needle and reattempt at a different interspace
- 19. Collect 1ml of CSF in each of 3 vials for: Tube 1: culture & gram stain Tube 2: glucose, protein Tube 3: cell count & differential and extra CSF if desired for other lab tests
- 20. Once the needle is removed, a small bandage is placed over the hole in your skin and you will be asked to remain flat on the exam table for a minimum of 30 minutes to help prevent any leakage of spinal fluid after the procedure. You will be encouraged to drink extra fluid while you recover and for the next two to three days. A headache following spinal tap occurs in up to 20 percent of patients. It typically occurs upon standing and is relieved by lying down. You should lie flat on your back or stomach (but not your side) for as long as you can the first 24 hours after the procedure or if you have a headache.
- 21. Also, to minimize complications, it is recommended that patients avoid bending and heavy lifting for two to three days following the procedure. Even lifting a small child following this procedure can cause the clot formation to become dislodged, resulting in a headache. Your provider will tell you when it is safe to return to work. Most people can generally return to work in one to two days. Wash hands Recording and reporting.
- 22. Headache Apnea (central or obstructive) Back pain Bleeding or fluid leak around spinal cord Infection, pain, hematoma Subarachnoid epidermal cyst Ocular muscle palsy (transient) Nerve Trauma
- 23. So today we have discuss the topic lumbar puncture under this we have discussed: Introduction, Anatomy of spine, Definition, Indications, Risk factors, Contraindications, Preparation of patient, Procedure, After care of patient.
- 24. Lumbar puncture is the process of insertion of a needle into lumbar region of the spine so that the cerebrospinal fluid can be withdrawn for laboratory investigations to diagnose the disease. It is a common procedure in order to detect any bacterial, viral infection causes the disease.