SSlleeeepp-- WWaakkee CCyyccllee
WWhhaatt iiss nnoorrmmaall ??
Sleep enters through NREM (slow wave sleep)
Alternates with REM about every 90 minutes
SWS in first 1/3 rd of night and REM in last 1/3rd
REM peaks in early hours of morning which coincides
with trough of body temperature
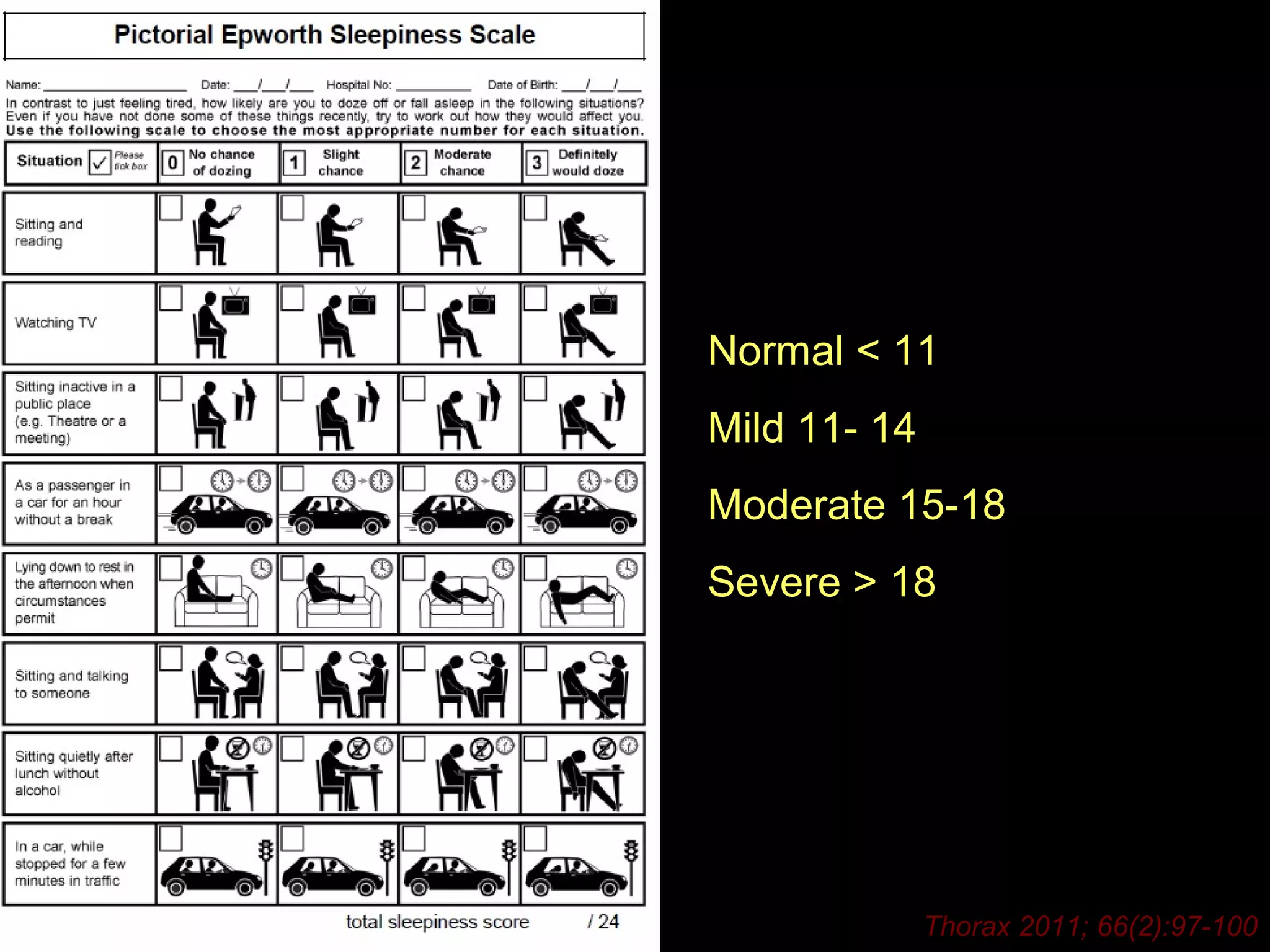
Epworth sleepiness Score
Best available tool to guide clinicians to patient
perception of sleepiness
Predicts level of compliance with CPAP
Guides to urgency of assessment
24.
Normal < 11
Mild 11- 14
Moderate 15-18
Severe > 18
Thorax 2011; 66(2):97-100
25.
Treatment options
Improve upper airway:
Weight reduction, tonsillar surgery, Bariatic surgery
CPAP: acts as a pneumatic splint (Compliance !!!)
Dental devices (‘MAD’):
As good as CPAP in mild-moderate OSA, better tolerated
Surgery:
UPPP, RF tissue reduction, Tracheotomy
Others:
Avoid alcohol, sleep on side (‘tennis balls’, postural alarm,
special pillows)
26.
Adherence to CPAP
Non-compliance: use < 4 hours a night (30% - 80%)
Adherences during the first week…
Severity of OSA (a weak relationship)
Degree of day time sleepiness (strong relationship)
Level of education….
Psychological traits: optimism, motivation to engage in
healthy behaviour ( ‘healthy user effect’)
Association of OSAwith
Hypertension
JAMA:2012;307:2169
37% developed HT at 12 years
Dose response effect
29.
Is CPAP usefulin
Hypertension ?.....Yes
BUT…..
Reduction in mean BP is only small
(- 2.5mm vs. + 0.8mm) at 4 weeks
Greater decrease among severe OSA (- 3.3mm)
Reduction in BP less than with anti-hypertensive
(Lorstatan vs. CPAP: -9mm vs. -2.1mm)
Reduction in BP is less in non-sleepy than in sleepy patients
Lancet 2002:359;204
AJRCCM 2010:182:954
30.
Effects of CPAPin HT with non-sleepy OSA
SBP reduced by -1.8 mm at 1 year DBP reduced by – 2.1mm
31.
CPAP more usefulin reducing BP in
sleepy than in non- sleepy OSA
In most studies patients who did not have excessive day
time drowsiness had NO reduction in the BP with CPAP
In sleepy patients benefits with CPAP seen even within 4
weeks of treatment, whereas non-sleepy patients need
CPAP for longer to achieve a smaller reduction in BP
32.
OSA and Coronaryheart disease:
The Sleep Heart Health study:
10 years follow up
1927 males 2495 females
OSA was predictor of incident CHD only in men, BUT after
adjustment for diabetes, lipids, hypertension and anti-hypertensive
medication use, the association was not
Circulation 2010:122:352-360
statistically significant in any group.
33.
OSA and CHD
Association of OSA with incident CHD
(Myocardial infarction, re-vascularisation and
coronary heart disease death)
is equivocal
34.
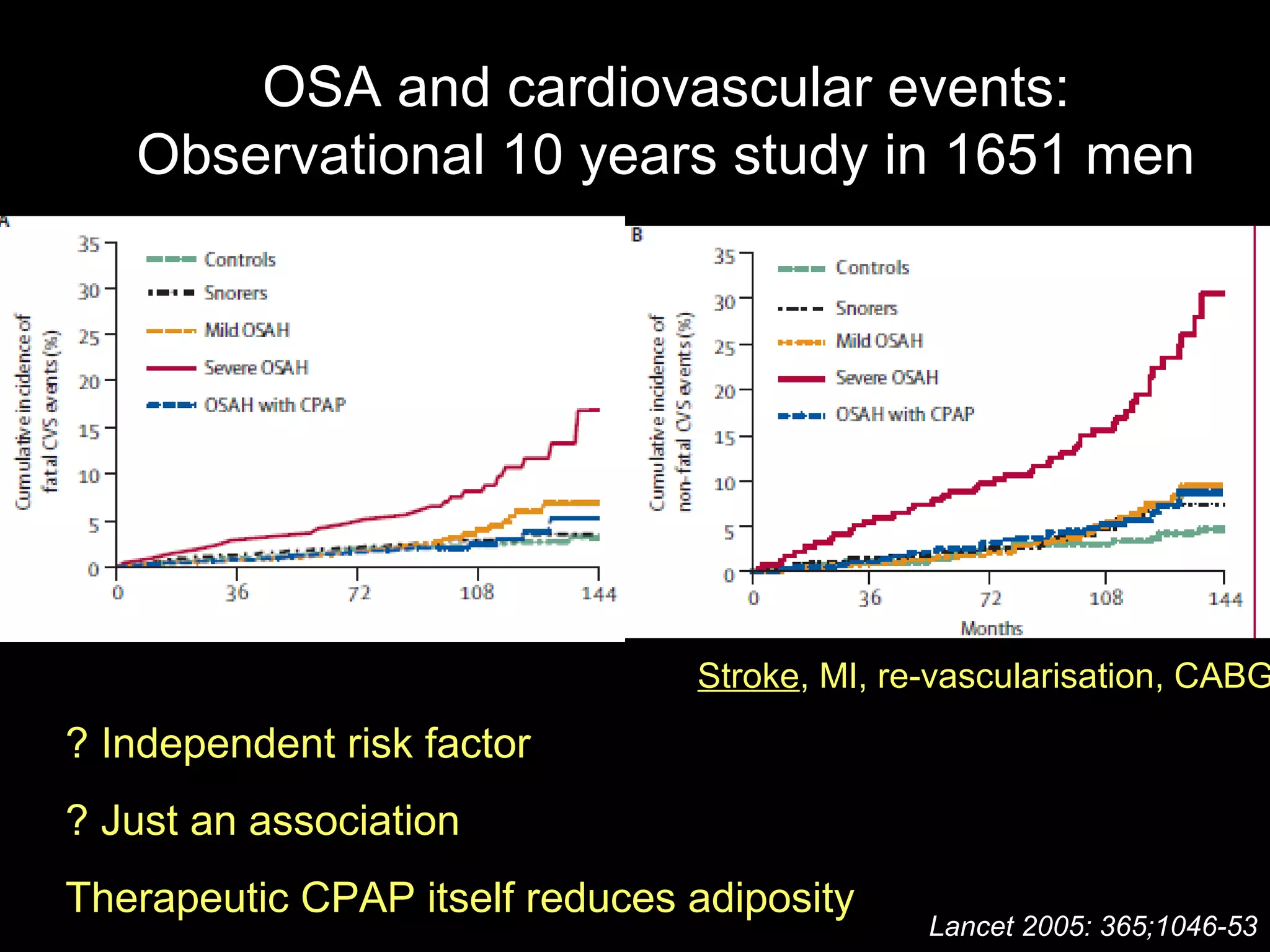
OSA and cardiovascularevents:
Observational 10 years study in 1651 men
Stroke, MI, re-vascularisation, CABG
Lancet 2005: 365;1046-53
? Independent risk factor
? Just an association
Therapeutic CPAP itself reduces adiposity
35.
OSA and Cardiovasculardisease
CPAP in severe OSA may reduce cardiovascular events
BUT…
No RCT that prove that CPAP improves mortality
No clinical trials to support routine use of CPAP in OSA
for sole purpose of reducing cardiovascular events
‘Healthy User effect’ could effect outcomes in studies
Chest 2010; Study of the healthy user effect in OSA
36.
OSA and Heartfailure:
The Sleep Heart Health study:
10 years follow up
1927 males 2495 females
OSA predicted incident heart failure in men but not in women
Circulation 2010:122:352-360
37.
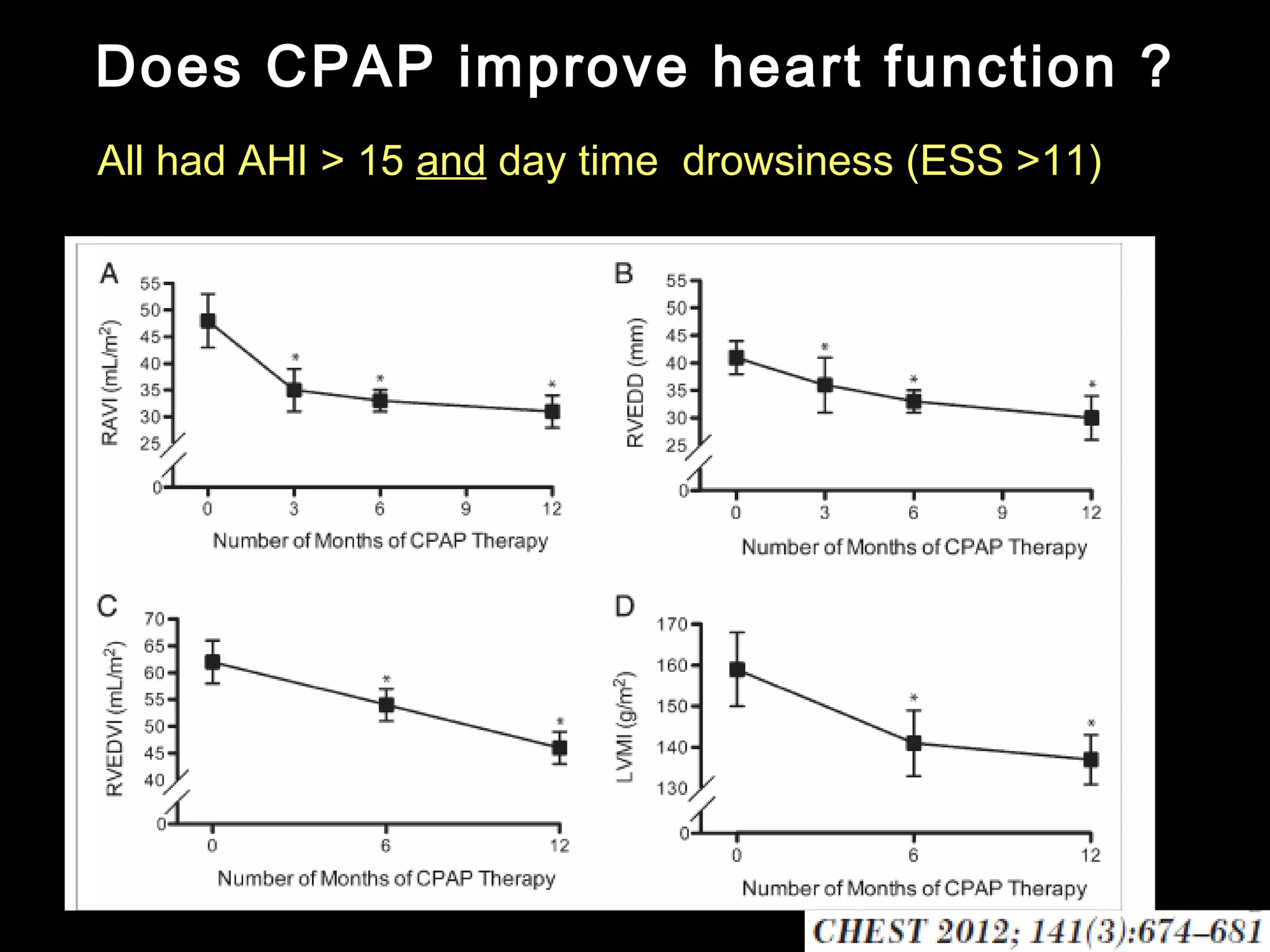
Does CPAP improveheart function ?
All had AHI > 15 and day time drowsiness (ESS >11)
38.
Does CPAP improveheart function ?
All had excessive day time drowsiness (ESS > 11)
No control group---- diet, exercise, changes in
medications and medication adherence could be
effected by close monitoring in the study
Natural history of CMRI in OSA is not known
CPAP adherence was 100% ( 52/52)
( “Healthy user effect”)
39.
OSA and arrhythmia
Recurrence of AF (at 1 year) after cardio version
Non OSA patients------- 52 % recurrence
Untreated OSA------ 82%
Treated with CPAP---- 42%
CPAP most useful for abolishing nocturnal ventricular
asystole and bradycardia ( ? effect on mortality)
If observed nocturnal arrhythmia– think OSA !!
40.
OSA and PulmonaryHT
Risk only if co-existent day time hypoxemia (i.e. associated
chronic lung disease)
Treatment with CPAP causes only very modest reduction in
PASP (from 29 mm to 24mm)
Eur Heart J 2006:27:1106
Evidence of improved mortality is lacking
Pulmonary HT alone is NOT an indication for diagnostic
evaluation of OSA
41.
Benefits of CPAPin OSA
The evidence !!
Decreased day time sleepiness
Improved quality of life
Improves cognitive function
Improves resistant hypertension
Improves heart function in heart failure
Reduces cardiovascular events
Improves metabolic abnormalities
Reduces mortality
?????
#4 Theta: low voltage- frequency 3-7 Hz
Sleep spindles- burst of sinuusodial waves called sleep spindles
delta-; high voltage slow frequency 0.5-2Hz
#6 In a young normal adult living in a conventional sleep wake cycle with no sleep complaints
REM sleep predominates in last 1/3rd of night and is linked to circadian rhythm of body temperature. It coincides with the trough of body temperature
#7 Low amplitute mixed frequency
Phasic events:
REM,
Irregularties with HR, respiration
#9 Sleep related cardiac events cause 20% of MI’s and 15% sudden cardiac deaths
NREM- reduced sympathetic tone and heightened Vagal tone- bradycardia, reduced CO, reduced BP so some autonomic instability– normally BP FALLS in NREM sleep
Aurosal from sleep also causes acute rise in NE causing raised BP
REM- autonomic instability, central release of Cholinergic surges and increased autonomic tone is responsible for SIDS, arrhythmias , reduced coronary blood flow due to HR rise, BP surges
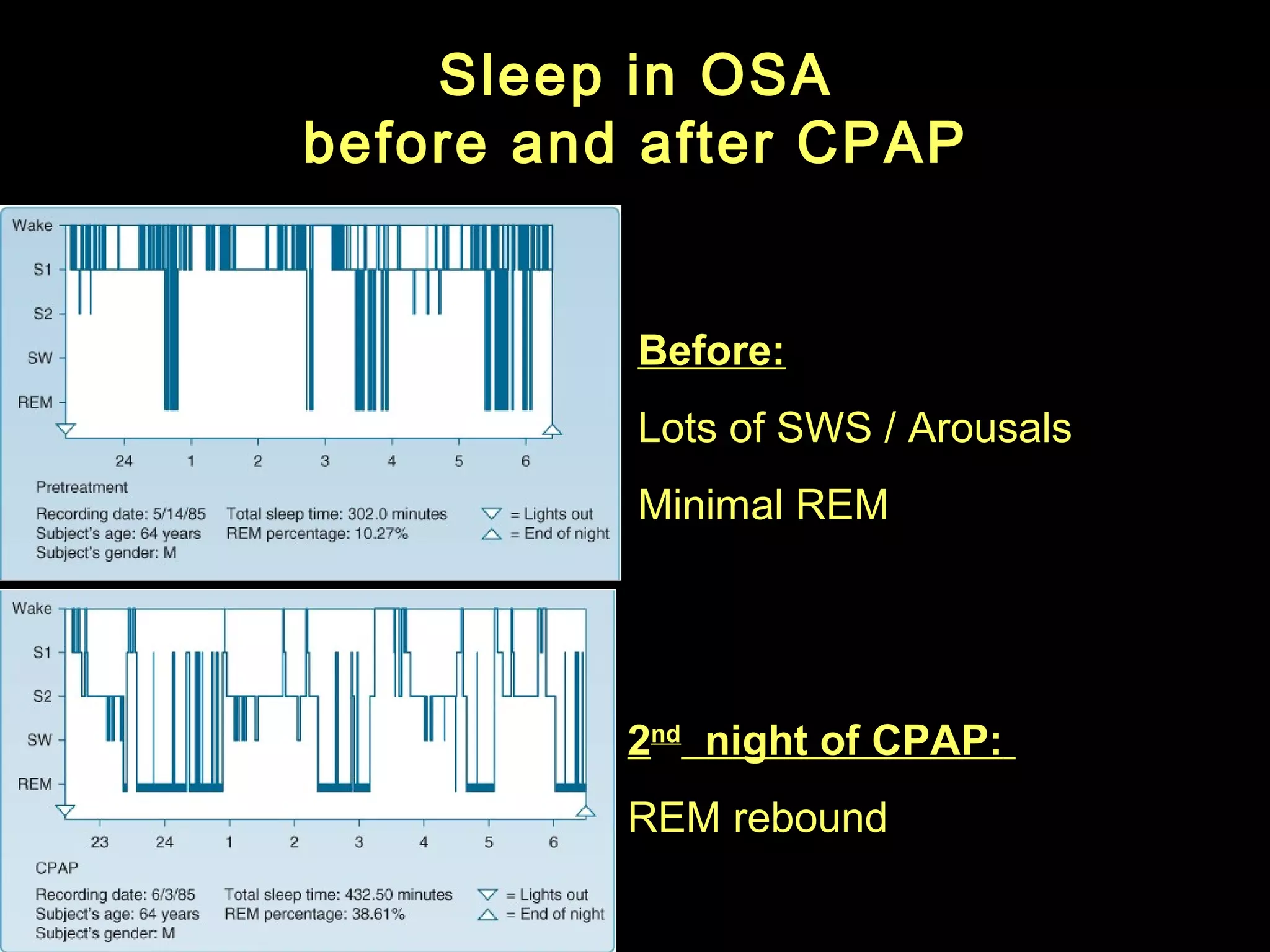
In OSA once treated with CPAP- SWS rebound during first night- can precipitate hypotension if patient on anti hypertensive
#10 Withdrawal of serotonergic and noradrenergic excitation on upper airways and increased cholinergic transmission
Suppression of activity of hypoglossal motor neurons so loss of tone of tounge
Reduced activity of geniohyoid and sternohyoid
#11 SWS extremely early biomarker of ageing of CNS. The decline of SWS begins around age 20. Human life expectancy was 20-30 years. Decline in SWS could be a evolutionary remnant of initiation of ageing
Healthy elderly people may not have any SWS
WASO( wake time after sleep onset)- increases with age- fragmented sleep
Older subjects shorter REM latency due to age dependent change in circadian timing systems. The core body temperature is phase advanced relative to sleep onset so early onset REM occurs
#12 If sleep loss for 1 or more nights
Ist night SWS recovers, 2nd night REM recovers
REM rebound during recovery ( eg OSA treated with CPAP- REM rebound- nightmares- increase REM related phenomenon&apos;s of either apnea during REM or REM hypoventilation)
if chronic sleep restriction- with recovery they get SOREM’s- can be associated with hallucinations/ sleep paralysis etc ( can mimic narcolepsy ) so sleep history important
TCA/MAO withdrawl- cause SOREMS
Alcohol- few pints
THC- cause ageing for there CNS, politicians do not believe
#13 Ist night SWS recovers– risk of hypotension
2nd night REM rebound– arrythemias, hypotension, hypoventilation ( C02 retention)
#14 4 imporatant muscles
genoglossus, genihyoid, sternohyoid- stabilises tongue/ hyoid
Tensor veli palati0 stabilises palate
Retroghathia they push mandible backward so narrow velopharynx
#15 Changes in the upper airways muscles during sleep
#16 The effort of breath which disturbs sleep and not the hypoxia ( seen in UARS– no hypoxia but arousal with flow limitation)
Lot of harms of OSA caused by sympathetic outflow
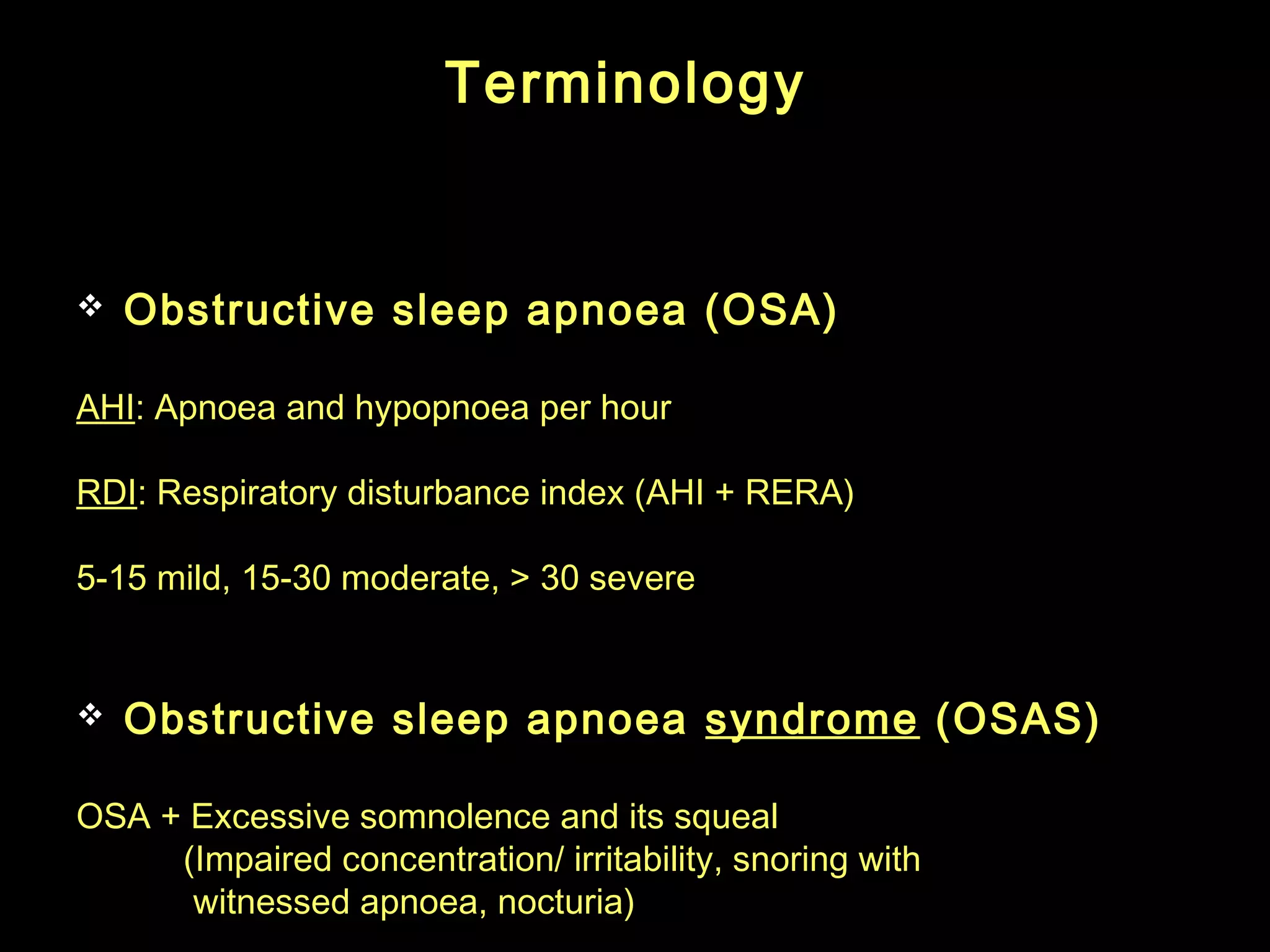
#17 Apnoea: No flow for 10 seconds
Hypopnea: A ≥30% drop from baseline in the nasal pressure transducer flow signal lasting at least 10 seconds and associated with a ≥4% desaturation
AHI; Number of A and H per hour
RERA: respiratory event related aurosals
RDI: AHI + RERA; RDI; 5-15 mild, 15-30 moderate, &gt; 30 severe– cut off arbitary
Nocturia due to either:Raised atrial natriuretic peptide levels from increased central blood volume, resulting from low intrathoracic pressures during obstructed breathing
The sleep fragmentation and disruption of the normal decrease in nocturnal urine production when asleep.
#19 Sleep fragmentation is due to repeated aurosaual and not due to low oxygen; Excessive somnolence, Impaired alertness, Poor cognition.
Drop in O2 and inappropiate intrathoracic pressure swings causies incrteased ventilatory drive cauisng arousal and sudden opening of the airways (gasp of air) and rise in oxygen saturation
Low oxygen causing pulmonary HT, arrythemias, polycenthemia etc
#21 More common in men due to different distribution of fat ( upper body obesity so incresaed neck circumfreence in men) compated to hip fat in women.
Large adenoid in childhood could also cause retardation of growth of mandible and predispose to OSA
Alcohol excaberates OSA, depresses CNS, worstens sllepiness, promotes weitht gain
Neuromuscular disoredres: stroke, myotonic or Duchenne dystrophy, and motor neurone disease.
Only OSA- rate is 24% in men and 9% women
#22 (measured with ESS)
Nocturia----
Raised ANP from increased central blood volume due to low intra-thoracic pressure during obstructed breathing
Sleep fragmentation causes disruption of normal decrease in urine production when asleep
#24 Other tools like Berlin questionnaire etc
More sleepy– high risk of accidents etc
#25 Good for patients with English as second language. Has been validated
33% participais made erreors while completing traditional ESS
75% preferred pictorial va traditional ESS 65%
#26 CPAP- problems of claustrophobia, nasal congestion, pain and ulceration of bridge of nose
UPPP- consists of removing part of the soft palate and tonsils and tightening up the side walls of the pharynx, are sometimes used in an attempt to improve snoring, although the benefit is unpredictable and limited- works ONLY IN MINORITY. However, a recent Cochrane review confirmed that it is not effective at treating obstructive sleep apnoea. [9]. It is also painful and can make subsequent use of nasal continuous positive airways pressure therapy more difficult. only partly successful in adults. PROBLEMS; Pian, nasal reflux, pharyngeal stenosis, dysphonia, infeection, bleeding.
Tonsillectomy and adenoidectomy can be curative in children
MAD– Protrude the mandible forward or hold tongue more anterior (Tounge retaining devices better tolerated in OSA and works by holding the lower jaw forward, patient MUST have his own teeth and is fitted by dentist
Problems with MAD: jaw discomfort. Dry mouth, slaivation. They are contraindicated in patients with loose fitting teeth, poorly controlled epilepsy, or temporomandibular joint problems.
#27 Many CPAP machines contain meters that record the duration that the machine is turned on. This approach is limited by its inability to differentiate the duration that the patient is receiving CPAP therapy from the duration that the machine is simply turned on and potentially not being used.
CPAP manufacturers provide several ways to obtain adherence data from the devices. As an example, a smart card can be inserted into the CPAP machine, removed by the patient, and taken or mailed to the provider&apos;s office to be read by a card-reader. Alternatively, the information can be transmitted by modem or wireless transmission. Provider-specific reports can then be generated, including graphic displays. The reports may include total device use, mean device use, and specific patterns of use.
No diffrence between auto-titration devices vs fixed pressure devices
#29 Spainish study with 1889 patients with OSA followed for 12 years– 37% developed HT
Incidence of HT was diagnosed with physician diagnosed HT and started on medications or BP of &gt; 140/90 recorded on 2 or more follow up visit separated by at least 1 week
There is a dose response effect:
Patients with mild OSA had twice the risk of controls and those with AHI &gt; 15 had three times risk that of controls
#30 BUT only 2mm reduction in BP is enough to reduce cardiovascular risks
Lancet randomly assigned 118 patients to use CPAP or sub-therapeutic CPAP for 1 month
Randomized cross over study: 23 patients with untreated HT and untreated OSA– measured mean 24 hours BP reading
Three out of 4 RCT that evaluated patients with OSA who did not have Excessive daytime sleepiness found NO reduction in the BP
Additional effect in patients already on anti-hypertensive
#31 725 patients with HT but ESS of &lt;11– 358 received CPAP and 367 no active treatment
(SBP reduced by -1.8mm and DBP by -2.1 mm after 1 year of
CPAP)
#32 Also benefits of CPAP seen earlier ( even at 4 weeks) in sleepy OSA
#33 Results—A total of 1927 men and 2495 women 40 years of age and free of coronary heart disease and heart
failure at the time of baseline polysomnography were followed up for a median of 8.7 years in this prospective
longitudinal epidemiological study. After adjustment for multiple risk factors, obstructive sleep apnea was a significant
predictor of incident coronary heart disease (myocardial infarction, revascularization procedure, or coronary heart
disease death) only in men less than 70 years of age– NOMINAL STATISTICAL SIFNIFICANCE (adjusted hazard ratio 1.10 [95% confidence interval 1.00 to 1.21] per
10-unit increase in apnea-hypopnea index [AHI]) but not in older men or in women of any age. Among men 40 to 70
years old, those with AHI 30 were 68% more likely to develop coronary heart disease than those with AHI 5.
COMMUNITY BASED SAMPLE
Conclusions—Its association with incident coronary heart disease in this sample is
equivocal. (
Association of OSA with CHD (MI, revascularisation, coronary heart disease death) was not statistically significant in either men or women after adjustment for covariates
Event rates increased with severity of OSA in men but NOT in women. After adjustment for age, race, BMI and smoking there was significant association of AHI with incident CHD in men but not in women BUT after adjustment for BM, lipids, BP and use of anti-0HT medications the association in men was NOT statistically significant
#35 1651 men followed for 10 years following PSG– OBSERVATIONAL STUDY
Patients with untreated severe OSA (mean AHI &gt; 42) had higher incidence of fatal and non-fatal CV events than untreated patients with mild-moderate OSA, patients treated with CPAP, simple snorers and healthy participants even after adjusting for confounding variables
This DOES NOT indicate causal relationship as severe OSA is associated with multiple vascular risk factors causing reduced HDL, increased CRP, increased homocuysteien, glucose etc
As viceral obesity itself is a risk factor for metabolic syndrome . Patients on CPAP also reduce there adiposity which could influence outcomes. It is still not clear if OSA is a further INDEPENDENT risk factor or merely an association
One problem is pooling of cerebro-vascular and cardiovascular disease. The studies suggest that OSA is greater risk of stroke rather than cardiovascular disease
#36 Severe OSA may also be associated with other multiple vascular morbidity– decreased HDL, increased CRP, rasied glucose, raised homocystiene all of which may not be corrected by use of CPAP
Non adhrenence to CPAP associated with non adherence to statins
Patients who adhere with CPAP are more likely to be healthier and have better compliance with drugs, diet etc than those who does not adhere with CPAP
Patients consistently refilling lipid lowering medications were more adherent to using CPAP
#37 Results—A total of 1927 men and 2495 women 40 years of age and free of coronary heart disease and heart
failure at the time of baseline polysomnography were followed up for a median of 8.7 years in this prospective
longitudinal epidemiological study.
Obstructive sleep apnea predicted incident heart failure in men but not in women (adjusted hazard ratio 1.13 [95% confidence interval 1.02 to 1.26] per 10-unit increase in AHI). Men with AHI 30 were 58% more likely to develop heart failure than those with AHI 5.
Conclusions—Obstructive sleep apnea is associated with an increased risk of incident heart failure in communitydwelling middle-aged and older men ( both less and more than 70 years age)
REASONS less in women
Less prevalence of OSA in women
Later age onset of OSA in women- usually post menopausal so LESS cumulative exposure to OSA
Men have greater ventilatory response to C02 and hypoxemia
Men have larger increase in LV mass for a given increase in BMI
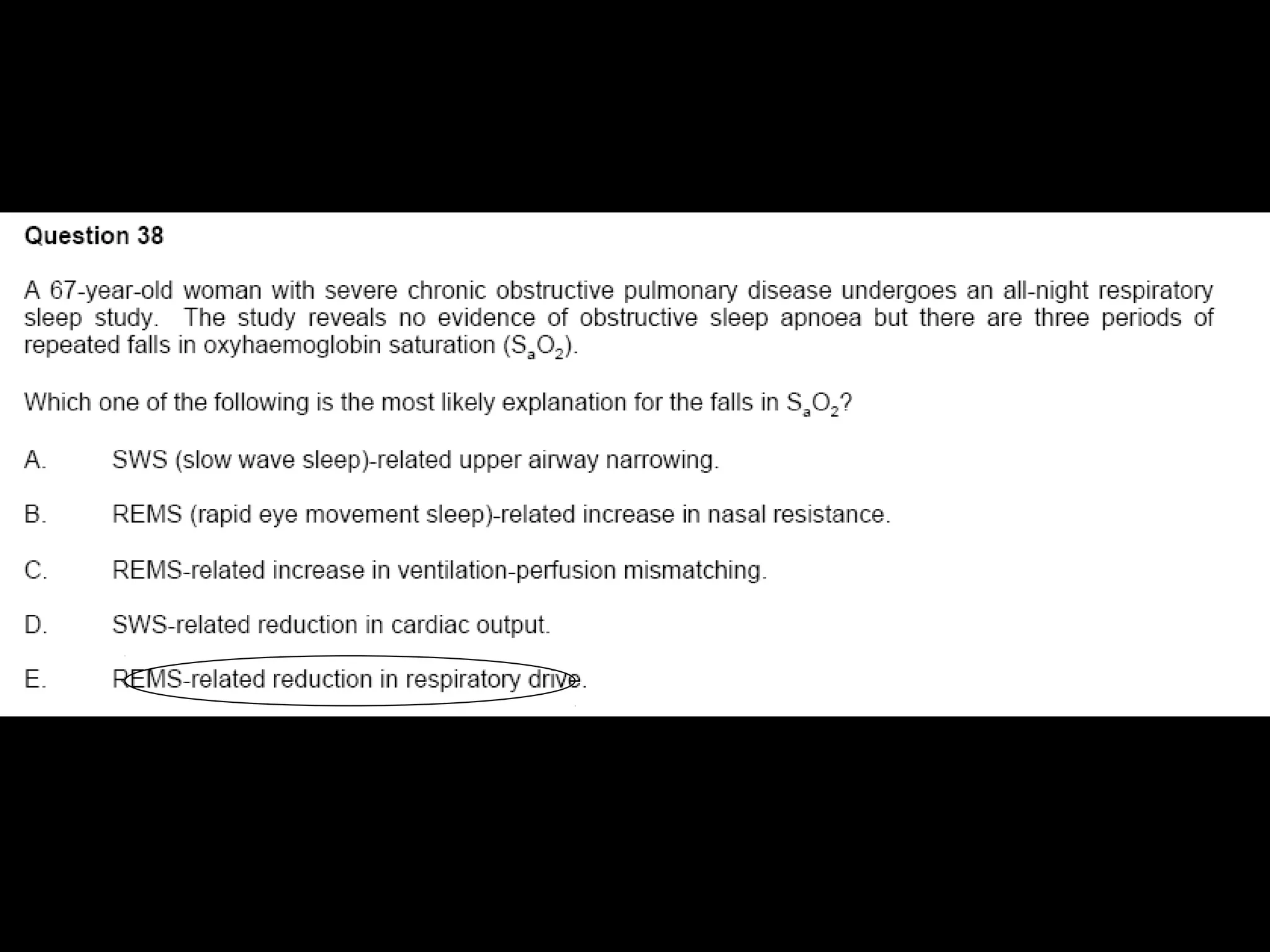
#38 All had AHI of &gt; 15 + day time drowsiness with ESS &gt; 10
Right atrial volume index, RV end diastolic volume index, RVEDD, LV mass as determined with CRM
No effects on pro BNP, CRP or TnT
LV mass predicts future events
Problems;
Uncontrolled study of 52 patients with no control group; The adherence to medications, diet, exercise could be effected by close monitoring
Natural history of CMR measurement in OSA is not known
CPAP adherence was HIGH in the group – ALL 52 were compliant for 1 year ( mean use of 4.5 H per night)
All had day time sleepiness- ESS &gt; 14, AHI &gt; 15
#39 Some changes could be unrelated to use of CPAP
#40 If observed nocturnal cardiac arrhythmia ( with or without day time arrhythmia) should be eveluated for possible OSA
#41 Isolated nocturnal hypoxemia NOT associated with cor pulmonmale
In study of 23 patinets with OSA randomly assigned to theurapatic CPAP vs subtheurapatic CPA for 12 weeks. The improvement in PASP was higest among patinets with OSA plus pulmonary HT
#42 Improves metabolic abnormalities– TC, LDL, TG, HbiAC, abdominal fat content, BMI -- NEJM 2011– CPAP for the metabolic syndrome in OSA– 3 months therapeutic CPAP then 3 months sham CPAP and other group vice versa. Problem was that CPAP group lost more weight as CPAP itself reduces adiposity ( less day tome drowsiness) so could effect outcomes
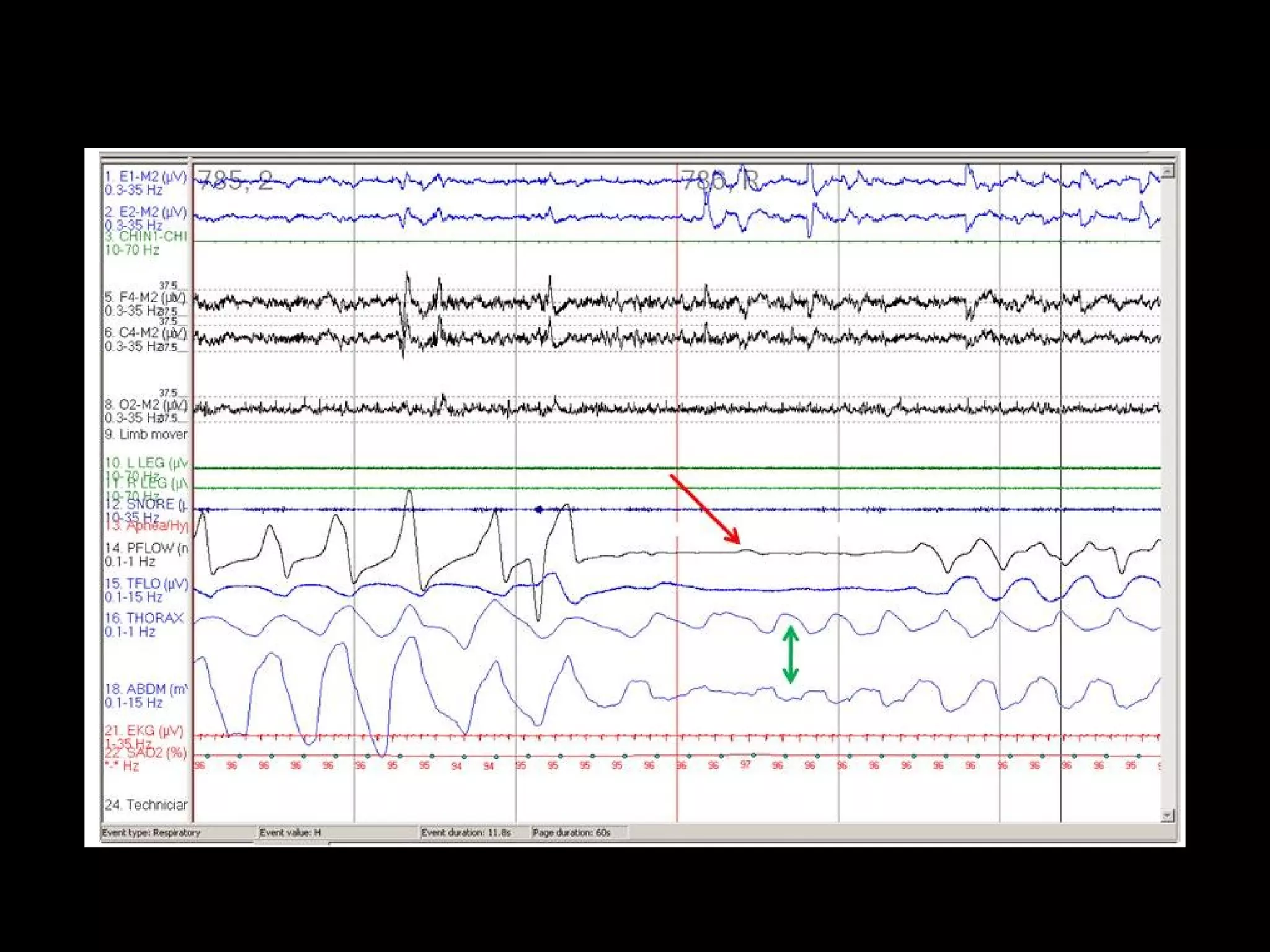
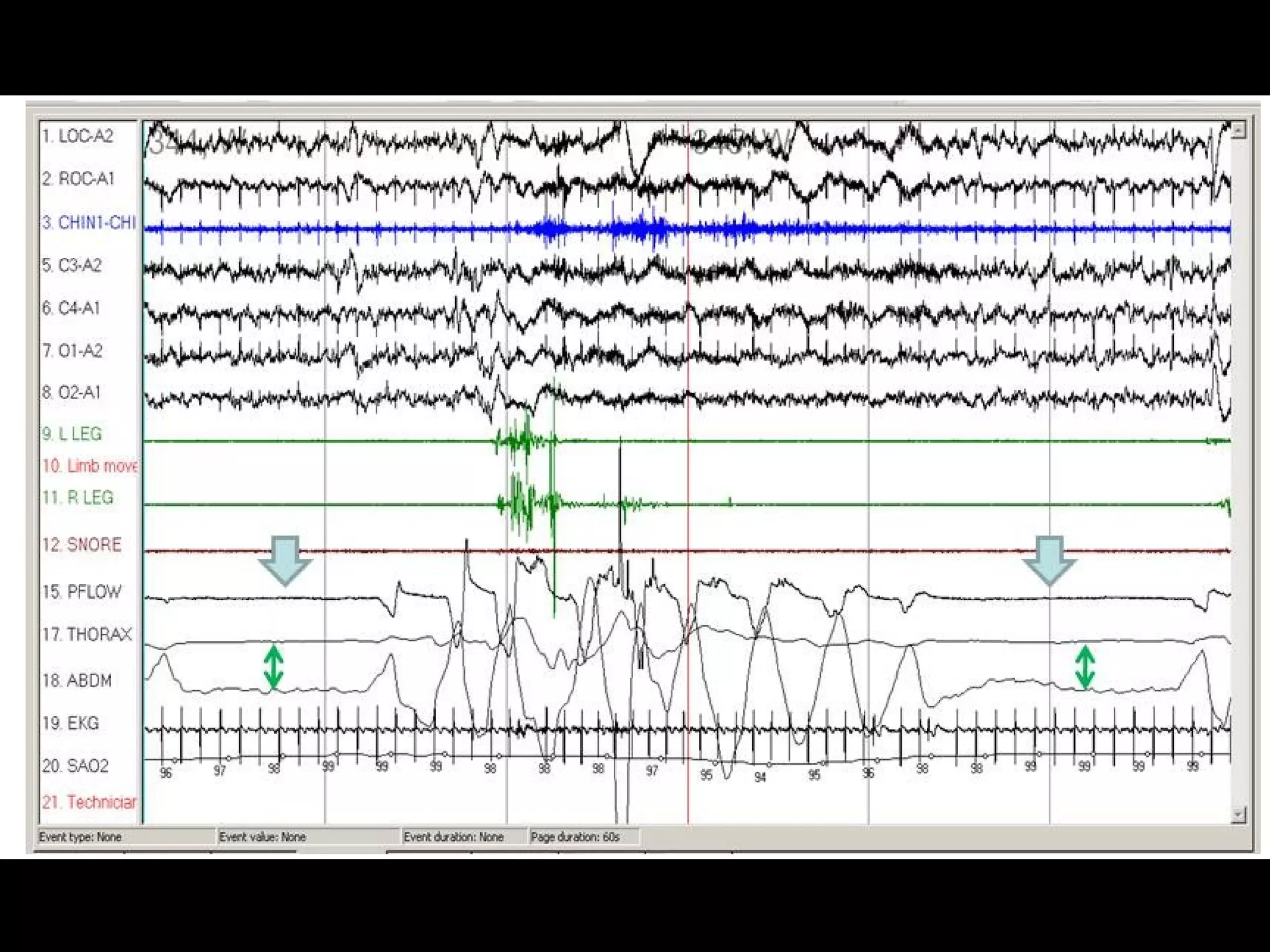
#43 Obstructive sleep apnea. Note the absence of flow (red arrow) despite paradoxical respiratory effort (green arrow).
#44 Comparison of a central apnea (box) and obstructive apnea (circle).
#45 Central sleep apnea (thick areas). Note the absence of both flow and respiratory effort (green double arrows).
Central apnea is the cessation of airflow for at least 10 seconds with no respiratory effort
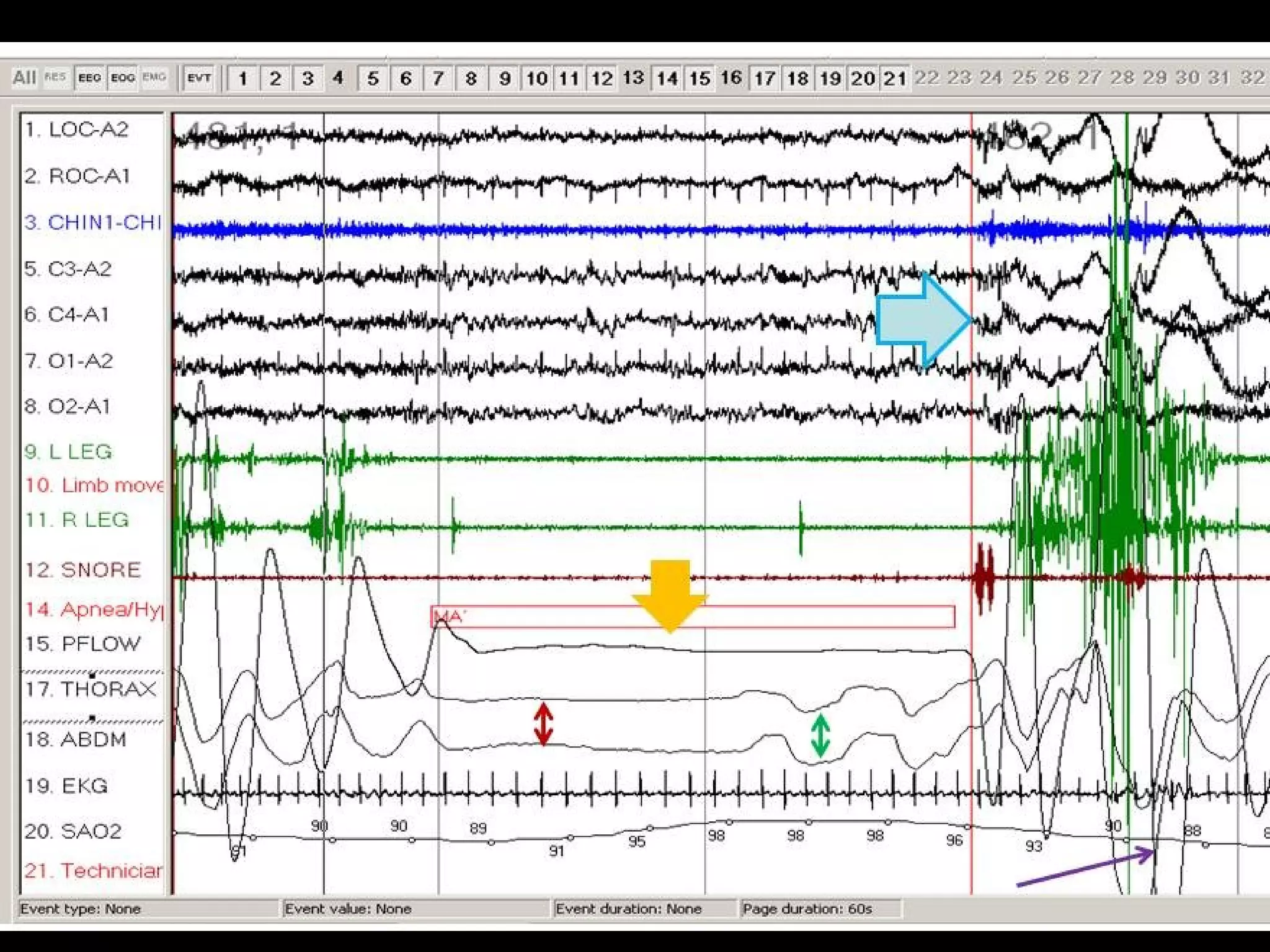
#46 Mixed sleep apnea. Note that the apnea (orange arrow) begins as a central apnea (effort absent; red double arrow) and ends as an obstructive apnea (effort present; green double arrow). Note the arousal (blue arrow) that terminates the apnea and the desaturation (purple arrow) that follows
#48 Peroidic breathing at sleep wake transition.- Alternating hyperventilation and hypoventilation with apnea at nadir
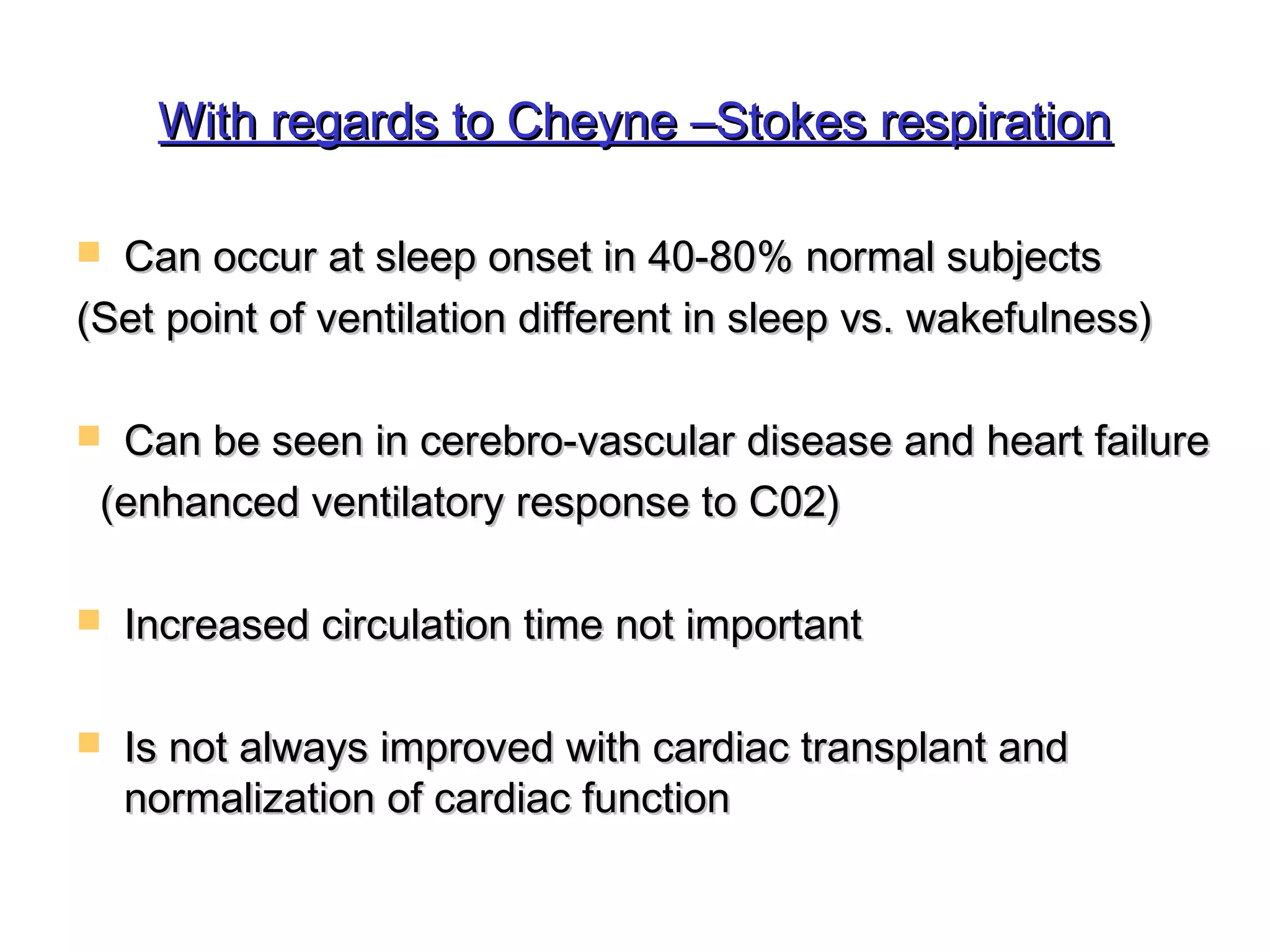
#49 Incidence of peroidic breathing at sleep onset 40-80% of normal subjects. This increases with age
Reason- set point of regulation on ventilation is different during wakefullness and sleep. During sleep reduced ventilation and pc02 rises adjusted to the sleep set point- on aurosal the increased pc02 above the wakefullness setpoint constitutes an error signal that causes hyperventilation ( increased ventilatory response to C02) until the c02 falls below wakefullness set point
In HF- enhanced ventilatory response to c02- acute increase in ventilation during aurosal, c02 falls below threshold- apnea- increased circulation time not impoprant and CSR not improved with cardiac transplant and normalization of cardiac function
CSR sustained by-enhanced ventilatory drive, pulmonary congestion, aurosals, apnea induced hypoxia
#52 REM- autonomic instability, central release of Cholinergic surges responsible for SIDS, arrhythmias , reduced coronary blood flow due to HR rise, BP surges
NREM- reduced sympathetic tone and heightened vagal tone so bradycardia
In OSA once treated with CPAP- SWS rebound during first night- can precipitate hypotension if patient on anti hypertensives
#55 However, patients with OHS have an elevated serum bicarbonate level due to the metabolic compensation for the chronic respiratory acidosis.
It was recently shown that serum bicarbonate combined with the severity of obstructive sleep apnea (OSA) can be used as clinical predictors of OHS in patients with severe obesity and OSA
OHS= Hyper-capnic OSA
OHS is defined as a combination of obesity (BMI &gt;= 30kg/m2) and awake chronic hypercapnia (PaCO2 &gt;= 45 mm Hg) accompanied by sleep-disordered breathing.
#56 In approximately 90% of patients with OHS the sleep-disordered breathing consists of obstructive sleep apnea (OSA).
OHS is labelled as sleep hypoventilation and is defined as an increase in PaCO2 during sleep by 10 mm Hg above wakefulness or significant oxygen desaturation that is not explained by obstructive apneas or hypopneas.3
#57 MSLT is for narcolepsy: would only be clinically indicated if daytime hypersomnolence persists after successful treatment with PVV
The test consists of four or five, twenty minute nap opportunities that are scheduled about two hours apart.
Positive if mean REM latency of &lt; 8 minutes with 2 REM onset naps( but just presnece of SOREM is not diagnostic of narcolepsy
Test negative if patient cannot sleep as excessive daytime sleepiness occurs in 100% of narcolepsy
#59 All of the symptoms listed are consistent with the diagnosis of narcolepsy, but only cataplexy is pathognomonic for narcolepsy.
Cataplexy occurs when skeletal muscle atonia is triggered by strong emotion such as laughter, anger, surprise, or excitement. The atonia results in muscle weakness in the in limbs, face, and neck. Episodes are generally brief (&lt; 2 minutes) and consciousness is generally preserved.
#61 MSLT is for narcolepsy
The test consists of four or five, twenty minute nap opportunities that are scheduled about two hours apart.
Positive if mean REM latency of &lt; 8 minutes with 2 REM onset naps( but just presnece of SOREM is not diagnostic of narcolepsy
Test negative if patient cannot sleep as excessive daytime sleepiness occurs in 100% of narcolepsy
The MWT is generally used to determine if a patient is able to stay awake during soporific conditions
The MWT consists of four sleep trials with breaks lasting for two hours in between them. You are not allowed to do other things to try and keep yourself awake. This includes actions such as singing or slapping your face. If you fall asleep, then you will be awakened after sleeping for only about 90 seconds. The test will end if you do not fall asleep within 40 minutes
A total of 97.5% of normal sleepers stay awake for an average of eight minutes or more during the MWT. Falling asleep in an average of less than eight minutes during the test would be considered abnormal. Results show that from 40% to 59% of people with normal sleep stay awake for the entire 40 minutes of all four trials
#62 excessive daytime sleepiness occurs in 100% of narcolepsy