
Recommended
Recommended
More Related Content
Similar to Counselling Psychology QuarterlyVol. 24, No. 1, March 2011, .docx
Similar to Counselling Psychology QuarterlyVol. 24, No. 1, March 2011, .docx (20)
More from voversbyobersby
More from voversbyobersby (20)
Recently uploaded
Recently uploaded (20)
Counselling Psychology QuarterlyVol. 24, No. 1, March 2011, .docx
- 1. Counselling Psychology Quarterly Vol. 24, No. 1, March 2011, 43–53 How special are the specialties? Workplace settings in counseling and clinical psychology in the United States Greg J. Neimeyer a*, Jennifer M. Taylor a , Douglas M. Wear b and Aysenur Buyukgoze-Kavas c a Department of Psychology, University of Florida, P.O. Box 112250, Gainesville, FL 32611, USA; b Psychology and Community Counseling Clinic, Antioch University Seattle, Seattle, WA 98121, USA; c Department of Educational Sciences, Division of Psychological
- 2. Counseling and Guidance, Middle East Technical University, Ankara, Turkey (Received 1 February 2010; final version received 18 February 2011) How special are the specialties? Although clinical and counseling psychol- ogy each have distinctive origins, past research suggests their potential convergence across time. In a survey of 5666 clinical and counseling psychologists, the similarities and differences between their workplace settings were examined during early-, mid-, and late-career phases to explore the distinctiveness of the two specialties. Overall, clinical and counseling psychologists reported markedly similar workplace settings. However, some significant differences remained; a greater proportion of counseling psychologists reported working in counseling centers, while a greater proportion of clinical psychologists reported working in medical settings. In addition, during late-career, substantially more counseling and clinical psychologists worked in independent practice contexts than in community mental health centers, medical settings, academia, or university counseling centers. Findings are discussed in relation to the ongoing distinctiveness of the two specialties and the implications of
- 3. this for training and service in the field of professional psychology. Keywords: clinical psychology; counseling psychology; workplace settings Introduction Recognized as distinct specialties by the American Psychological Association, clinical and counseling psychology each have distinct histories, intersecting appli- cations, and longstanding concerns regarding their continuing, or diminishing, differences. This article explores these issues and examines the contemporary similarities and differences between these two specialties as reflected in their workplace settings. Workplace settings are examined at early, mid, and late career in order to determine whether differences vary by cohort in a way that might reflect either on their enduring or diminishing differences over time. Enduring or diminishing differences? Historically, the specialties of clinical and counseling psychology have developed from different origins and formed distinctly different trajectories as a result *Corresponding author. Email: [email protected] ISSN 0951–5070 print/ISSN 1469–3674 online � 2011 Taylor & Francis DOI: 10.1080/09515070.2011.558343
- 4. http://www.informaworld.com (Munley, Duncan, McDonnell, & Sauer, 2004). Clinical psychology drew heavily from the mental health movement that emphasized psychological dysfunction, disability, and rehabilitation (McFall, 2006). Its alignment with the medical model, which places a premium on assessment, diagnosis, and treatment within a broad range of hospital and community contexts, reflects a coherent extension of the specialty across time (Tipton, 1983). Counseling psychology, by contrast, derived largely from the vocational guidance movement that emphasized the productive matching of a person to his or her work environment in the interest of optimizing performance and satisfaction (McFall, 2006; Munley et al., 2004). Counseling psychology’s enduring commitment to vocational psychology, personal adjustment, multiculturalism, and social justice (Neimeyer & Diamond, 2001; Tipton, 1983) can be seen as an ongoing testament to the person–environment fit that animated its origins over a century ago (Whiteley, 1980). These historical differences are reflected in a range of contemporary distinctions between the two specialties, as well (Munley et al., 2004). Longstanding literatures have addressed the enduring distinctions between clinical and
- 5. counseling psychology training programs in relation to their theoretical commitments (Norcross & Prochaska, 1982; Ogunfowora & Drapeau, 2008) and their training models (Korman, 1974; Norcross, Kohout, & Wicherski, 2005), and have sought to see whether these differences translate into differential internship placements (Brems & Johnson, 1996; Neimeyer & Keilin, 2007; Neimeyer, Rice, & Keilin, 2009; Shivy, Mazzeo, & Sullivan, 2007) or workplace experiences (Owens, Moradi, & Neimeyer, 2008). Early work concerning their theoretical preferences noted substantial differences between clinical and counseling psychology. Some of the most preferred orientations within the field of counseling psychology, such as Rogerian, humanistic and existen- tial, were among the least preferred orientations within clinical psychology (Norcross & Prochaska, 1982; Watkins, Lopez, Campbell, & Himmell, 1986). By contrast, behavioral and psychodynamic theories have been found to be preferred within clinical training programs (Bechtoldt, Norcross, Wyckoff, Pokrywa, & Campbell, 2001). These theoretical differences have been noted among students and practi- tioners (Cassin, Singer, Dobson, & Altmaier, 2007), as well as among the training directors in these respective specialties (Norcross, Sayette, Mayne, Karg, & Turkson, 1998).
- 6. Other work, however, has suggested diminishing differences between the specialties in this regard over time (Zook & Walton, 1989). The majority of students and professionals within both of these specialties recently have been found to identify themselves as eclectic, integrative, or cognitive-behavioral (Bechtoldt et al., 2001), for example, with only modest differences in relation to identification with psychoanalytic, behavioral, or humanistic orientations. The recent work of Ogunfowora and Drapeau (2008) reported no significant differences between the two specialties in relation to any of the theoretical orientations they studied, including humanistic, psychodynamic, behavioral, or biological approaches. In addition to exploring potential theoretical differences, research on the distinctiveness of clinical and counseling psychology has also noted increasing distinctions in relation to their underlying training models. Historically, both clinical and counseling psychology positioned themselves beneath the scientist–practitioner training model (Norcross, Castle, Sayette, & Mayne, 2004). With its distinctive emphasis on the integration of science and practice, the Boulder Model (1949) 44 G.J. Neimeyer et al.
- 7. dominated the field professional of training within both specialties until the introduction of the Scholar–Practitioner model that arose from the Vail conference (1973). The scholar–practitioner model was introduced as an alternative to the scientist–practitioner model (Korman, 1974), placing primary emphasis on profes- sional training and on the interpretation and application of research, rather than its generation or dissemination. The scholar–practitioner model of training has proliferated rapidly within clinical psychology, but not within counseling psychology (Norcross et al., 2005). Today, the modal degree conferred in the field of clinical psychology is a Psy.D. degree, which serves as a strong testament to the appeal of the scholar– practitioner model within the field of clinical psychology. By contrast, counseling psychology has retained its longstanding commitment to the scientist–practitioner training model, viewing it as core to its identity as a specialty (Stoltenberg et al., 2000). Unlike clinical psychology, counseling psychology has only two Psy.D. programs, for example, and has regularly reaffirmed its longstanding commitment, the Boulder training model (Meara et al., 1988; Murdock, Alcorn, Heesacker, & Stoltenberg, 1998). A number of researchers have sought to explore the implications of these differences between clinical and counseling psychology and to
- 8. determine whether or not they translate into differential outcomes. Taylor and Neimeyer (2009), for example, found qualitative differences in mentoring between clinical and counseling psychology training programs. Students in counseling programs were generally more satisfied and reported higher levels of socioemotional mentoring, but somewhat lower levels of research productivity. Brems and Johnson (1996) studied the internship placements of clinical and counseling students and found that more clinical students were placed in health science centers than were counseling students, whereas more counseling students were placed in university counseling centers, and these findings were supported in a 30-year retrospective of internship placements within the field of counseling psychology in the United States (Neimeyer & Keilin, 2007). The recent work of Neimeyer et al. (2009) extends these findings. In comparing the internship placements for an entire cohort group of clinical and counseling psychology students, they found differences that mirrored previous findings; against a background of considerable similarity, clinical psychology students nonetheless were significantly more likely to obtain internships in hospital and medical center contexts, whereas counseling psychologists more commonly were placed within counseling center contexts. Some provisional evidence also supports the idea that these
- 9. differences may translate into workplace differences, as well. Watkins et al. (1986), for example, found that counseling psychologists were more often employed in counseling centers and academic departments, whereas clinical psychologists were more often found in private practice and medical settings (see also Watkins, Schneider, Cox, & Reinberg, 1987), findings that were largely replicated by the subsequent work of Zook and Walton (1989) and Brems and Johnson (1996). Likewise, Bechtoldt et al. (2001) found that clinical psychologists were more likely to be employed in private practice, hospitals and medical schools, while counseling psychologists were more likely to be employed in counseling centers, differences that have been noted in more recent research, as well (Mogan & Cohen, 2008). Despite these differences, however, there is longstanding concern that counseling psychology may be losing ground in relation to preserving the distinctiveness of its specialization. The sometimes subtle differences in theoretical orientations within Counselling Psychology Quarterly 45 counseling and clinical, for example, occur against the background of substantial theoretical similarity (Cassin et al., 2007). And, while differences in training models
- 10. clearly persist, a number of researchers have asked, ‘‘Does the model matter?’’ and some concluded that it may not (cf. Neimeyer et al., 2007; Rodolfa, Kaslow, Stewart, Keilin, & Baker, 2005). The convergence of the specialties is reflected most clearly, perhaps, in the recognition that most counseling psychology graduates do not emphasize their distinctiveness. Instead, they refer to themselves generically as ‘‘clinical practi- tioners’’ (Watkins et al., 1986), a finding that raises additional concerns about the diminishing distinctiveness of the specialties in the professional marketplace. In fact, Mosher (1980) and Fitzgerald and Osipow (1986) suggest that counseling psychology may either become extinct or simply become absorbed into clinical psychology, most notably because psychologists from both camps are experiencing a convergence in terms of their workplace settings. The purpose of this research was to examine the workplace settings of clinical and counseling psychologists for the evidence of this convergence or of their continuing distinctiveness. By examining these workplace differences within early- mid- and late-career professionals, we hoped to determine whether any differences between the specialties have increased or decreased across the various cohort groups. Methods
- 11. Participants In cooperation with the State, Provincial and Territorial Psychological Associations (SPTAs), an Internet survey of psychologists was conducted across North America. Executive Directors of the Associations were solicited through the Council of Executives of State and Provincial Psychological Associations (CESPPA). Those who agreed to participate were provided with an email to forward to their memberships that described the nature of the study and included a link to the informed consent and survey, which could be completed and submitted online. This survey was part of a larger study that examined broader perceptions of professional development (Neimeyer, Taylor, & Wear, 2009), which included a range of demographic questions, such as the area of one’s degree type (clinical or counseling psychology), workplace setting (Community Mental Health Center, Hospital or Medical Setting, Independent Practice, University Academic Department, University Counseling Center or Mental Health Service, or Other), and the year the highest degree was conferred, among other demographic questions. A total of 5666 psychologists (clinical n¼4182; counseling n¼1484) responded to the survey. Fifty-four of the 58 licensing jurisdictions were represented, for a participation rate of 93.1% of the jurisdictions. The overall membership of the
- 12. SPTAs is approximately 40,000 members, meaning that the current sample represented approximately 14.2% of the total population of the collective member- ships. In all, 58.5% of the participants were women and 41.5% were men. The mean age of participants was 52.7 (SD¼11.79), which closely approximates the mean age of APA members (54.3 years). The majority of the sample reported their ethnicity as White/Caucasian (91.7%), followed by Hispanic (2%), African American (1.7%), Asian (1.2%), two or more races (1.0%), Other (0.8%), American Indian or Alaskan (0.2%), or Native Hawaiian (0.2%); 1.1% declined to report their ethnicities. 46 G.J. Neimeyer et al. The percentages of ethnic minorities in the sample closely approximate the percentages of psychologists represented in the membership of APA, where 2.1% are Hispanic, 2% are Asian, 1.8% are African American, and 0.2% are American Indian, and 0.4% are multiracial (Center for Psychology Workforce Analysis and Research, 2007). In terms of workplace setting, the majority of participants described themselves as working in independent practice (56.6%), followed by hospital/medical settings (15.0%), community mental health settings (7.6%), academic settings (6.9%), university counseling center settings (5.0%), or other
- 13. (8.9%). Participants represented a relatively experienced sample of psychologists, with the median date of licensure being 1989 (SD¼10.97). Approximately 16.4% of participants (n¼926) were considered in their ‘‘early career’’ phase (0–7 years post- highest degree), 39.1% of participants (n¼2210) were considered in their ‘‘mid-career’’ phase (8–20 years post-highest degree), and 44.5% of participants (n¼2518) were considered in their ‘‘late career’’ phase (21 or more years post-highest degree). Procedures Participants were asked to read the Informed Consent describing the study. After indicating their consent to participate, individuals were linked to the survey. Participants completed and submitted their surveys online anonymously. The survey included questions regarding specialty (clinical or counseling) and current workplace setting. Results and discussion Chi-square statistics were conducted to determine if there were significant differences in workplace settings across the career phases of those who graduated from clinical and counseling psychology programs. Pearson Chi-square statistics indicated significant differences between the two specialties in relation to workplace settings in early career, �2(5, N¼907)¼27.77, p 5 0.001, in mid-career
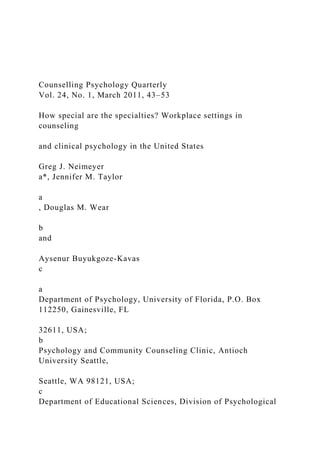
- 14. �2(5, N¼2175)¼ 65.72, p 5 0.001, and in late career, �2(5, N¼2461)¼67.50, p 5 0.001, phases. These differences emerged against the backdrop of substantial similarities between the workplace profiles of the two specialties, however. As illustrated in Figure 1, the profiles of workplace settings for clinical and counseling psychologists were generally quite similar at each career stage. For example, within community mental health centers (CMHCs), 13.7% of clinical psychologists and 14.8% of counseling psychologists in the early career phase reported working in this setting. Likewise, in mid-career, 7% of clinical psychologists and 8.3% of counseling psychologists worked in this setting, percentages that diminished somewhat during late career both for the clinical (5.6%) of clinical psychologists work in CMHCs, and counseling psychologists (4.9%). Unlike CMHC’s, however, more substantial workplace differences occurred in relation to hospital or medical settings, particularly in early career. At early career, nearly one-quarter (24.4%) of clinical psychologists reported working in hospitals or medical settings, compared with 17.7% of the counseling psychologists. At mid- career, the percentages were comparable for clinical (16.8%) and counseling (17.3%). At late career, both groups showed a substantial decline, though the decline within
- 15. Counselling Psychology Quarterly 47 clinical psychology (13.2%) was greater than the decline within counseling psychology (9.5%). For both clinical and counseling psychologists, independent practice was the predominant workplace setting across all stages of the career. However, unlike all other workplace settings, the percentage of clinical and counseling psychologists in independent practice appears to have increased, rather than to have decreased, from early to late career. Nearly twice as many clinical psychologists in late career (66.4%) reported working in independent practices when compared to clinical psychologists working in independent practices in earlier stages of their career (38.7%). Similar findings are observed with counseling psychologists, where 60% of late career counseling psychologists reported working in independent practices, compared with only 35.4% of early career counseling psychologists. It is noteworthy, however, that a higher percentage of clinical psychologists reported working in independent practice settings during each of the three career stages. Regarding academic setting, similarities between clinical and counseling psy-
- 16. chologists were again found. In the early career stage 7.7% of the clinical psychologists reported working in an academic setting, compared with 5.7% in mid-career and 6.7% in late-career. For counseling psychologists, the percentage of academic work settings was similarly consistent across early (7%), mid (7.2%), and late (9%) career phases though, as reported by Cassin et al. (2007), a larger percentage of counseling psychologists were employed in academic settings overall (Watkins et al., 1987). Perhaps, the most striking differences between clinical and counseling psychology occurred in relation to university counseling center settings, where counseling psychologists predominated at each career stage. In each phase, the percentage of counseling psychologists working in counseling center contexts was more than three times that of clinical psychologists. Counseling psychologists in early (16.0%), mid (11.6%), and late (8.2%) phases of their careers were consistently more strongly represented in this work setting compared to clinical psychologists (5.6% in early, 3.2% in mid, and 1.8% in late career), though both groups showed a decline in workplace representation from early to late career. 100 Early Career Clinical 80
- 17. 90 , Mid-Career, Clinical Late Career, Clinical 60 70 Early Career, Counseling Mid-Career, Counseling 40 50 Late Career, Counseling 20 30 0 10 Hospital or Academic SettingCommunity Mental Health Center Medical Setting
- 18. Independent Practice University Counseling Center Figure 1. Workplace differences by specialty across career trajectories. 48 G.J. Neimeyer et al. The overall pattern of these results provides qualified support for the distinc- tiveness of clinical and counseling psychology in relation to the workplace settings of the professionals within those fields. Against a backdrop of substantial similarity, the differences that did emerge were consistent with the distinctive values of the respective specialties. Clinical psychologists, for example, were more strongly represented in medical and hospital settings, at least early in their careers, and counseling psychologists were more heavily represented in counseling center settings throughout their careers. This profile of workplace settings may help inform students who seek graduate training in professional psychology. This could prove valuable
- 19. given the recent work of Cassin et al. (2007) which suggests that students’ anticipations regarding their future employment may diverge substantially from the actual settings in which graduates find employment. Cassin et al. (2007), for example, found that 33% of counseling psychology graduate students anticipated academic careers, whereas the data from this study indicate that in early career, only 5.7% of counseling psychologists had academic placements. Likewise, only 7.7% of early career clinical psychologists were in academic contexts, compared with 20.1% of the clinical students who anticipated academic careers (Cassin et al., 2007). By contrast, in relation to independent practice, the picture is reversed. Fewer counseling students (24.2%) and clinical students (26.6%) anticipate going into independent practice than are represented in early career, where 35.4% of the counseling psychologists and 38.7% of the clinical psychologists find employment. Thus, this study suggests that students may benefit from gaining a more realistic sense of their workplace probabilities and, perhaps, even utilize this information in their decision making regarding the particular specialty they prefer to pursue. For aspiring graduate students who want to work within a counseling center setting, for example, it may be useful to know that counseling psychologists are disproportionately employed by counseling centers, and this may provide useful information
- 20. when considering which graduate schools to apply to. It is important to emphasize, however, that clinical and counseling psychologists are represented in each of the workplace settings included in this study, so employment opportunities are available to both across all of these workplace contexts. Moreover, with few distinctions, the profiles of workplace settings were quite similar for clinical and counseling psychologist across the various cohort groups. Although clear cohort-related shifts occurred, with more professionals in independent practice in late career (cf. Zook & Walton, 1989), these shifts did not appear to vary by specialty. In short, there was no evidence that the differences between clinical and counseling psychology were either substantially greater or lesser in early than in late career. Evidence of stronger late career differences, but diminishing mid and early career differences, might have been consistent with the idea that the differences between the specialties are diminishing across time (Fitzgerald & Osipow, 1986). However, no such evidence was found within this study. To the contrary, the patterns of workplace settings for clinical and counseling psychologists were largely consistent across cohort groups. Overall, the results of this study provide qualified support for the distinctiveness of clinical and counseling psychology, as reflected in the
- 21. workplace settings of their practitioners. While substantial differences were the exception, rather than the rule, those differences that did emerge clearly conformed to stipulated differences between the specialties and seemed to endure across cohort groups. Counselling Psychology Quarterly 49 It is important to underscore, though, that the examination of workplace settings provides only a global indicator of possible workplace differences. As Owens et al. (2008) have demonstrated, clinical and counseling psychologists within the same workplace setting can have strikingly different experiences and they fulfill different functions (Tipton, 1983), as well. Within the same setting the duties that are fulfilled and the orientations that are expressed by clinical and counseling psychologists may be markedly different (Osipow, 1980). Zook and Walton (1989), for example, found that while clinical psychologists more often approached their work from a psychodynamic approach, counseling psychologists commonly
- 22. utilized a humanistic approach toward their work. Importantly, these differences would be masked in this study where only differences in the workplace setting itself were examined, rather than functions and orientations and perspectives expressed within that workplace. For this reason, the results of this study are best regarded as providing a conservative picture of the differences between the two specialties, leaving it to future work to develop a more detailed picture of the distinctions between the specialties, not only in relation to the places of their employment, but also in relation to the duties, functions, and orientation that each brings to its workplaces. In addition, it is important to underscore that the cohort differences examined in this study do not necessarily reflect developmental differences. The fact that substantially more clinical and counseling psychologists appear in independent practice contexts during late career, for example, could reflect a movement across the
- 23. career trajectory away from other workplace settings and toward independent practice. Alternatively, it may simply reflect a cohort effect, with more late-career individuals spending their entire careers in independent practice contexts, while early career individuals have taken positions in more diverse occupational contexts. Although cohort differences between clinical and counseling psychology were not evident in this sample, it nonetheless remains for future longitudinal efforts to address any genuine developmental differences between the specialties that may have occurred across time. A final caveat has to do with the rapid internationalization of counseling psychology (Munley et al., 2004; Takooshian, 2003). As the specialty of counseling psychology makes systematic progress toward its international development (Leong & Ponterotto, 2003; Leung, 2003), this development will likely register its effects on workplace settings associated with professionals within this field, as well. A number
- 24. of researchers and scholars have noted important variations as a function of the cultural adaptation of the specialty to a range of international contexts (Kavas, Taylor, & Neimeyer, 2010; Pelling, 2004; Takooshian, 2003), and these may well be reflected in workplace settings, as well, as the field continues its process of globalization. Indeed, the rapid globalization of the specialty, as well as its quest to embrace cultural diversity and variation, may become a further feature that distinguishes it as a specialty (Neimeyer & Diamond, 2001). Within the context of these considerations, however, this study provides provisional evidence regarding the continuing differences between clinical and counseling psychology training programs in relation to one of their principal outcomes: the workplace settings of the professionals they train. Future work that clarifies the nature and implications of these differences may contribute to a better understanding of the contemporary distinctions between these
- 25. specialties. And these distinctions may, in turn, serve as the basis for more informed and effective decision 50 G.J. Neimeyer et al. making on the part of students whose career interests may be shaped by the knowledge of the contexts in which they might eventually work. Notes on contributors Greg J. Neimeyer received his PhD in counseling psychology from the University of Notre Dame. He is professor of psychology in the Department of Psychology at the University of Florida and Director of the Office of Continuing Education and Psychology at the American Psychological Association. A fellow of the American Psychological Association, he is also a member of the Department of Community Health and Family Medicine where he conducts his clinical practice. His areas of research include professional development, epistemology and psychotherapy, constructivism, social influence in clinical contexts, and relationship development and disorder. Jennifer M. Taylor received her MS in counseling psychology from the University of Florida. She is currently a PhD candidate in the University of Florida counseling psychology program. Her research focuses on professional development and
- 26. competencies, continuing education, and mentoring. Douglas M. Wear received his PhD in clinical psychology from the University of Wyoming. He is the president of Wear & Associates, Inc., executive director of the Washington State Psychological Association, director of Antioch University Seattle Psychology and Community Counseling Clinic, chair of the APA Continuing Education Committee, and past chair of APA Council of Executive Directors of State and Provincial Psychological Associations. His research and professional interests include professional development, supervision, manage- ment, consulting, and coaching. Aysenur Buyukgoze-Kavas is a research assistant and PhD student at Middle East Technical University, Psychological Counseling and Guidance program. She is part of the Scientific HR Development Program, which aims to train future academicians of Turkey. As a part of this program, she worked as a visiting research scholar at University of Florida, Department of Psychology from February 2009 to October 2009. She is a member of the Turkish Psychological Counseling and Guidance Association and American Psychological Association Division 17. Her major research interests are career decision-making, career indecision, counseling supervision, mentoring and job satisfaction. References
- 27. Bechtoldt, H., Norcross, J.C., Wyckoff, L.A., Pokrywa, M.L., & Campbell, L.F. (2001). Theoretical orientations and employment settings in clinical and counseling psychologists: A comparative study. The Clinical Psychologist, 54, 3–6. Brems, C., & Johnson, M.E. (1996). Comparison of Ph.D. programs in clinical and counseling psychology. Journal of Psychology, 130, 485–500. Cassin, S.E., Singer, A.R., Dobson, K.S., & Altmaier, E.M. (2007). Professional interests and career aspirations of graduate students in professional psychology: An exploratory survey. Training and Education in Professional Psychology, 1, 26–37. Center for Psychology Workforce Analysis and Research. (2007). Demographic characteristics of APA members by membership status. Retrieved July 25, 2009, from http:// research.apa.org/profile2007t1.pdf Fitzgerald, L.F., & Osipow, S.H. (1986). An occupational analysis of counseling psychology: How special is the specialty? American Psychologist, 41, 535– 544. Kavas, A., Taylor, J.M., & Neimeyer, G.J. (2010). Mentoring in counseling psychology: A cross-cultural comparison of students in the United States and
- 28. Turkey. Unpublished manuscript, University of Florida, Gainesville, Florida. Counselling Psychology Quarterly 51 Korman, M. (1974). National conference on levels and patterns of professional training in psychology: The major themes. American Psychologist, 29, 441–449. Leong, F.T.L., & Ponterotto, J.G. (2003). A proposal for internationalizing counseling psychology in the United States: Rationale, recommendations and challenges. The Counseling Psychologist, 31, 381–395. Leung, S.A. (2003). A journey worth traveling: Globalizaiton of counseling psychology. The Counseling Psychologist, 31, 412–419. McFall, R.M. (2006). Doctoral training in clinical psychology. Annual Review of Clinical Psychology, 2, 21–49. Meara, N.M., Schmidt, L.D., Carrington, C.H., Davis, K.L., Dixon, D.N., Fretz, B.R., Myers, R.A., & Suinn, R.M. (1988). Training and accreditation in counseling psychology. The Counseling Psychologist, 16, 336–384.
- 29. Mogan, R.D., & Cohen, L.M. (2008). Clinical and counseling psychology: Can differences be gleaned from printed recruiting materials? Training and Education in Professional Psychology, 2, 156–164. Mosher, R. (1980). On beating dead horses. The Counseling Psychologist, 8, 16–18. Munley, P.H., Duncan, L.E., McDonnell, K.A., & Sauer, E.M. (2004). Counseling psychology in the United States of America. Counselling Psychology Quarterly, 17, 247–271. Murdock, N.L., Alcorn, J., Heesacker, M., & Stoltenberg, C. (1998). Model training program in counseling psychology. The Counseling Psychologist, 26, 658–672. Neimeyer, G.J., & Diamond, A.K. (2001). The anticipated future of counseling psychology in the United States: A Delphi poll. Counselling Psychology Quarterly, 14, 49–65. Neimeyer, G., & Keilin, G. (2007). Tracking trends: A longitudinal look at internship placements in counseling psychology in the United States. Counselling Psychology Quarterly, 20, 123–134. Neimeyer, G., Rice, K.G., & Keilin, W.G. (2009). Internship placements: Similarities and
- 30. differences between clinical and counseling psychology programs. Training and Education in Professional Psychology, 3, 47–52. Norcross, J.C., Castle, P.H., Sayette, M.A., & Mayne, T.J. (2004). The PsyD: Heterogeneity in practitioner training. Professional Psychology: Research and Practice, 35, 412–419. Norcross, J.C., Kohout, J.L., & Wicherski, M. (2005). Graduate study in psychology. American Psychologist, 60, 959–975. Norcross, J.C., & Prochaska, J.O. (1982). A national survey of clinical psychologists: Affiliations and orientations. Clinical Psychologist, 35, 1–4. Norcross, J.C., Sayette, M.A., Mayne, T.J., Karg, R.S., & Turkson, M.A. (1998). Selecting a doctoral program in professional psychology: Some comparisons among PhD counseling, PhD clinical, and PsyD clinical psychology programs. Professional Psychology: Research and Practice, 29, 609–614. Ogunfowora, B., & Drapeau, M. (2008). Comparing counseling and clinical psychology practitioners: Similarities and differences on theoretical orientations revisited.
- 31. International Journal for the Advancement of Counselling, 30, 93–103. Osipow, S.H. (1980). Toward counseling psychology in the year 2000. The Counseling Psychologist, 8, 18–19. Owens, G., Moradi, B., & Neimeyer, G. (2008). Work-related perceptions of faculty in clinical and counseling academic training programs. Psychology Journal, 5, 25–39. Pelling, N. (2004). Counselling psychology: Diversity and commonalities across the Western world. Counselling Psychology Quarterly, 17, 239–245. Rodolfa, E.R., Kaslow, N.J., Stewart, A.E., Keilin, W.G., & Baker, J. (2005). Internship training: Do models really matter? Professional Psychology: Research and Practice, 36, 25–31. Shivy, V.A., Mazzeo, S.E., & Sullivan, T.N. (2007). Clinical and counseling psychology doctoral trainees: How students perceive internships. Training and Education in Professional Psychology, 1, 163–173. 52 G.J. Neimeyer et al. Stoltenberg, C.D., Pace, T.M., Kashubeck-West, S., Biever, J.L., Patterson, T., & Welch, I.D.
- 32. (2000). Training models in counseling psychology: Scientist- practitioner versus practitio- ner-scholar. The Counseling Psychologist, 28, 622–640. Takooshian, H. (2003). Counseling psychology’s wide new horizons. The Counseling Psychologist, 31, 420–426. Taylor, J.M., & Neimeyer, G.J. (2009). Graduate school mentoring in clinical, counseling, and experimental academic programs: An exploratory study. Counselling Psychology Quarterly, 22, 257–266. Tipton, R.M. (1983). Clinical and counseling psychology: A study of roles and functions. Professional Psychology: Research and Practice, 14, 837–846. Watkins, C.E., Lopez, F.G., Campbell, V.L., & Himmell, C.D. (1986). Contemporary counseling psychology: Results of a national survey. Journal of Counseling Psychology, 33, 301–309. Watkins II, C.E., Schneider, L.J., Cox, J.R.H., & Reinberg, J.A. (1987). Clinical psychology and counseling psychology: On similarities and differences revisited. Professional Psychology: Research and Practice, 18, 530–535. Whiteley, J.M. (1980). Counseling psychology in the year 2000 A.D. The Counseling Psychologist, 8, 2–8.
- 33. Zook II, A., & Walton, J.M. (1989). Theoretical orientations and work settings of clinical and counseling psychologists: A current perspective. Professional Psychology: Research and Practice, 20, 23–31. Counselling Psychology Quarterly 53 Copyright of Counselling Psychology Quarterly is the property of Routledge and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use. The Narrowing of Theoretical Orientations in Clinical Psychology Doctoral Training Laurie Heatherington, Williams College Stanley B. Messer, Rutgers University Lynne Angus, York University Timothy J. Strauman, Duke University
- 34. Myrna L. Friedlander, University at Albany Gregory G. Kolden, University of Wisconsin The focus of this article is the increasingly narrow range of therapeutic orientations represented in clinical psychology graduate training programs, particularly within the most research-oriented programs. Data on the self-reported therapeutic orientations of faculty at “clinical science” Ph.D. programs, Ph.D. programs at comprehensive universities in clinical and in counseling psychology, Psy.D. programs at comprehensive universi- ties, and Ph.D. or Psy.D. programs at freestanding spe- cialized institutions reveal a strong predominance of faculty with cognitive-behavioral orientations at the more science-focused programs, and a narrower range of orientations than in the more practice-focused pro- grams. We discuss the implications of this trend for the future development of clinical psychology and provide suggestions for addressing the attendant concerns.
- 35. Key words: CBT hegemony, clinical training and research, theoretical orientation. [Clin Psychol Sci Prac 19: 362–374, 2013] The growth of our knowledge is the result of a process closely resembling what Darwin called ‘natural selection’; that is, the natural selection of hypotheses: our knowledge consists, at every moment, of those hypotheses which have shown their (comparative) fitness by surviving so far in their struggle for existence; a competitive struggle which eliminates those hypotheses which are unfit. Karl Popper (1979) The best way to have a good idea is to have a lot of ideas. Linus Pauling Doctoral training in clinical psychology is clearly in a state of evolution. The scientist–practitioner (“Boul- der”) model that characterized the training landscape since 1949 has been challenged by several strong ideo- logical and sociological forces and developments. Argu-
- 36. ments for the value of more practice-focused doctoral training led to the development of Psy.D. programs, beginning in the 1970s. Subsequently, market forces have resulted in the explosive growth of large, prac- tice-focused doctoral training programs at freestanding institutions, dubbed “specialized institutions not offer- ing comprehensive education beyond psychology or counseling” by Sayette, Norcross, and Dimoff (2011, p. 4), and hereafter referred to as “specialized institu- tions,” as well as a crisis in the oversupply of applicants relative to the availability of doctoral internships (Munsey, 2011; Vasquez, 2011). Controversies about standards for doctoral training programs, especially with regard to the need to teach evidence-based treatments (Bray, 2011; Calhoun, Moras, Pilkonis, & Rehm, Address correspondence to Laurie Heatherington, Ph.D., Department of Psychology, Williams College, Williamstown, MA 01267. E-mail: lheather[email protected]
- 37. © 2013 American Psychological Association. Published by Wiley Periodicals, Inc., on behalf of the American Psychological Association. All rights reserved. For permission, please email: permissionsuk.wiley.com 364 1998; Davison, 1998; Eby, Chin, Rollock, Schwartz, & Worrell, 2011), continue. And most recently, the assertion by some that current American Psychological Association (APA) accreditation standards and practices are undermining the science of clinical psychology has resulted in the creation of alternative accreditation stan- dards that emphasize research and clinical training focusing on empirically supported treatments and assessment (Baker, McFall, & Shoham, 2009; McFall, 2007). The outcomes of this evolution in training are difficult to predict, and the relative merits of the vari- ous training models are a matter of widely diverging opinions and beyond the scope of this article. However, a recent study of APA-accredited clinical
- 38. Ph.D. programs (Sayette et al., 2011), including the Academy of Psychological Clinical Science (APCS, 2012) 1 and non-APCS programs in regular (“compre- hensive”) university settings and in specialized universi- ties, but excluding Psy.D. and counseling psychology Ph.D. programs, demonstrated a number of significant differences in acceptance rates, numbers of applicants admitted, admissions credentials, extent of financial aid, student demographic characteristics, and program fea- tures (e.g., research funding, internship acceptance rates). The study also found stronger faculty allegiance to a cognitive-behavioral orientation in APCS pro- grams (80%), as compared with non-APCS programs (67%) and programs in the specialized institutions (37%), as well as stronger allegiances to psychodynamic and humanistic/existential orientations in non-APCS versus APCS programs.
- 39. This article expands and critically discusses the latter finding. We argue that the finding regarding theoretical orientation reflects a feature of the evolving training landscape that is central to the future of clinical psy- chology but which has received little formal attention, that is, the increasingly restricted range of therapeutic orientations that clinical graduate students are expected to draw upon in their professional work. We contend that an unfortunate effect of some otherwise positive developments in promoting clinical psychology as a sci- ence is the danger of a monoculture of ideas about the nature of psychotherapeutic change—specifically, a hegemony of cognitive-behavioral theory and therapy. Furthermore, this effect is moderated by the nature of the doctoral training program. That is, the more research-based, science-focused programs tend to offer the narrowest range of theoretical orientations, whereas the more practice-focused programs present the widest ones. In this article, we present data suggesting that this
- 40. divide is evident within doctoral programs at compre- hensive universities, especially in clinical psychology (but not counseling psychology) programs. The divide is particularly evident when comparing clinical programs at comprehensive universities versus programs at freestanding professional schools of psychology. Following the presentation of data supporting this assertion, we discuss the dangers of these divides. First, however, consider the following thought exer- cise. Imagine that you are the mentor of a talented undergraduate who is beginning the clinical psychology doctoral application process. She has a strong liberal arts preparation, with a range of psychology courses in both clinical and nonclinical areas, and good research experience. She plans a career that includes psychother- apy research and theory development, and she wants solid clinical training as well. She is compiling an initial list of programs and is particularly interested in family
- 41. systems theory and therapy. As her mentor, you consider programs with core faculty (those who supervise theses and dissertations, that is, excluding adjuncts, off-site practicum supervisors, faculty in departments of psychi- atry that do not offer doctoral degrees) who publish research in addition to providing clinical training. Now, repeat the exercise with humanistic, experiential or existential theory/therapy, with psychodynamic theory/ther- apy, and with interpersonal theory/therapy. Having done this exercise ourselves and having mentored students like this one, we are aware of the difficulty in coming up with programs to suggest; indeed, these lists are likely to be very short. The data presented below bear out these personal observations. We undertook a systematic study of theo- retical orientations represented in clinical and counsel- ing doctoral training programs of various types, using published sources. The Insider’s Guide to Graduate
- 42. Programs in Clinical and Counseling Psychology (Sayette, Mayne, & Norcross, 2010) provided information on self-reported theoretical orientations of program faculty in six categories, that is, Psychodynamic, Behavioral, Family Systems, Cognitive Behavioral, Humanistic/ Existential, and Other; the guide allows for faculty to THEORETICAL ORIENTATIONS � HEATHERINGTON ET AL. 365 indicate one or more orientations. The APA’s 2010 Graduate Study in Psychology (APA, 2010) education/ accreditation web site (http://apa.org/ed/accreditation/ programs/index.aspx) and the list of member programs published by the Academy of Psychological Clinical Science (http://acadpsychclinicalscience.org/members) provided designations of various program types. As needed, Internet searches of individual programs were used to confirm their statuses as (a) Ph.D. programs at
- 43. comprehensive universities, (b) Ph.D. programs at comprehensive universities that are designated as clini- cal science programs, (c) Psy.D. programs at compre- hensive university programs, and (d) Psy.D. or Ph.D. programs at freestanding, “specialized” institutions. We included programs in the 50 U.S. states and Canada. Although the APA is phasing out accreditation of Canadian programs as of 2015, our concern is not with credentialing issues, but rather with training and con- tinued development in psychotherapy theory and research, which has been and no doubt will continue to be significantly influenced by Canadian psychology. For this same reason, we also included counseling psy- chology, but treated it separately, as virtually all coun- seling psychology doctoral programs are at comprehensive universities and because there are some historical and current differences between counseling and clinical psychology. Moreover, we excluded the
- 44. eight APA-accredited “combined” (e.g., school/clini- cal, school/counseling) programs. Table 1 presents the mean percentages of faculty in various types of clinical psychology doctoral programs who self-report particular theoretical orientations. 2 The comparison is striking. In the clinical science programs, fully 80% of faculty claim a cognitive-behavioral orien- tation, and 89% claim either a behavioral or cognitive- behavioral orientation, whereas small percentages of faculty claim either a psychodynamic or a humanistic/ existential orientation. Fewer than half of the faculty in Psy.D. programs at comprehensive universities and in Psy.D. or Ph.D. programs in freestanding universities claim a CBT orientation, with noticeably higher per- centages of faculty (28% and 29%, respectively) claim- ing a psychodynamic orientation. Interestingly, the least variation across programs was found in the per-
- 45. centages of faculty claiming a family systems orienta- tion, close to 20% of faculty in each type of program. Table 2 presents the mean percentages of faculty in counseling psychology doctoral programs who self- report particular theoretical orientations. These data reveal a wider range of orientations, with fewer than half claiming a behavioral or cognitive-behavioral ori- entation and nearly a third claiming a humanistic/exis- tential orientation. Explanations for this variation will be advanced shortly. Some elaboration and qualifications of these data are in order. First, in the Insider’s Guide, programs could also designate faculty with “other” orientations. These data were sparse and often unique to individual pro- grams or individual faculty and thus are not included in the table, but rather summarized as follows. Of the 54 clinical science programs, only two cited one or more “other” orientations. These (and the number of pro-
- 46. grams that cited them) were neuropsychology (1), community (1), interpersonal (1), motivational inter- Table 1. Therapeutic orientations of faculty in clinical psychology doctoral training programs Program Type Psychodynamic (%) Behavioral (%) Family Systems (%) Humanistic/Existential (%) Cognitivea Behavioral (%) Ph.D. programs designated as “clinical science”b programs (n = 54) 7 9 17 4 80 All other Ph.D. programs at comprehensive universities (n = 116) 19 11 20 24 67 Psy.D. programs at comprehensive universities (n = 31) 28 5 16 12 48 Psy.D. and Ph.D. programs at freestanding professional schools (n = 37) 29 6 22 15 32
- 47. Ms 21 8 19 14 57 a Source: Sayette et al. (2010). b Source: Academy of Psychological Clinical Science (http://acadpsychclinicalscience.org/index.php?page=members). CLINICAL PSYCHOLOGY: SCIENCE AND PRACTICE � V19 N4, DECEMBER 2012 366 viewing (1), child (1), and eclectic (1). Of the 116 other clinical Ph.D. programs at comprehensive univer- sities, 15 listed faculty with “other” orientations: health (1), integrative (3), community (1), clinical neuropsy- chology (3), eclectic (1), interpersonal or interpersonal/ ego relations or cognitive/interpersonal (5), develop- mental psychopathology (1), feminist (2), cognitive (1), narrative/personal construct (1). Of the 31 Psy.D. pro- grams at comprehensive universities, only one listed an “other” orientation: integrative/transtheoretical. Of the 38 programs at freestanding professional schools, four listed “other” orientations: research (1), integrative (2), cultural diversity focus (1). And of the 66 doctoral
- 48. counseling programs, 13 listed “other” orientations: eclectic (1), integrative (1), interpersonal (7), feminist/ multicultural or feminist or multicultural (13), con- structivist (2), relational/process (1), narrative (1), developmental systems (2). Second, the data on orientations in the Insider’s Guide were only available as percentages. We do not know how many actual faculty are represented in these percentages; “20%” of faculty claiming a family systems orientation could refer to one or two individuals in smaller programs, but several individuals in programs with larger faculties. Although the APA Graduate Study guide lists numbers of faculty, it was not possible (given changing faculty sizes, variability in the recency of the data in each source) to accurately compare the data in these two sources to derive the raw numbers of faculty. Nevertheless, this issue is of obvious importance, because it speaks to the actual availability of mentors
- 49. and supervisors representing particular orientations, as well as the viability of training and research from the particular theoretical orientation at any given program. Adding the percentages for each program, however, provides a rough index of the extent to which faculty at a particular program claim more than one allegiance, that is, eclectic orientations. That is, in programs at which each faculty member claims a single orientation, the mean percentages for each orientation total to 100%. For programs in which faculty members claim more than one orientation, the percentages total to more than 100%, with higher totals representing more faculty claiming multiple allegiances. The total percent- ages averaged across the different program types are the following: Ph.D. programs at comprehensive universi- ties, M = 129%, Ph.D. programs at comprehensive universities that are designated as clinical science pro- grams, M = 107%, Psy.D. programs at comprehensive university programs, M = 110%, Psy.D. or Ph.D. pro-
- 50. grams at the freestanding, “specialized” institutions, M = 105%, and counseling psychology doctoral pro- grams, M = 114%. Interestingly, the modal and median percentage totals were the same (each 100%) for every program type. SO WHAT? IMPLICATIONS FOR TRAINING, RESEARCH, THEORY, AND PRACTICE The data revealed two major divisions: between the types of theoretical orientations in which current stu- dents/future clinical psychologists are being trained and between the theoretical orientations predominant in the more research-focused and more practice-focused programs. These divides are potentially dangerous for the field and the future development of psychotherapy theory and research. It should be noted as well that the data revealed a third divide, between clinical and counseling psychol- ogy programs, which is noteworthy in that it provides some context for the current concern. The broader
- 51. theoretical focus in counseling psychology can be explained by differences in its history and training phi- losophies. Although counseling psychology training programs have required curricula and training experi- ences that are similar to those of clinical psychology programs, counseling psychology has different roots in Table 2. Therapeutic orientations of faculty in counseling psychology doctoral training programs Psychodynamic (%) Behavioral (%) Family Systems (%) Humanistic/ Existential (%) Cognitivea Behavioral (%) Ph.D. programs at comprehensive universities (n = 67) 19 1 18 31 42
- 52. a Source: Sayette et al. (2010). THEORETICAL ORIENTATIONS � HEATHERINGTON ET AL. 367 group career counseling, vocational rehabilitation of WWII veterans (Gelso & Fretz, 1992), and counseling of “normal” individuals with developmental difficulties or life problems (Friedlander, Pieterse, & Lambert, 2012). This history dovetails with the fact that the pre- dominant training model in counseling psychology for the last 45 years has focused on relationship-oriented and microcounseling skills (Egan, 2007; Hill, 2004; Ivey & Ivey, 2007; Ridley, Kelly, & Mollen, 2011). In practicum training, the preferred supervision approach is to foster trainees’ experience with a range of theoret- ical approaches, always being guided by clients’ indi- vidual problems and needs. Most counseling psychology programs do not hire faculty members based on theoretical orientation; rather, the prevailing
- 53. preference seems to be a faculty that represents a broad range of approaches. Further, reflecting the de-empha- sis on the medical model (matching treatment to diag- nosis) and the preferred emphasis on relationship skills and common factors, counseling psychology researchers have traditionally focused more on explicating thera- peutic change factors than on comparing client out- comes by treatment approach. Indeed, some of the historically most influential lines of psychotherapy pro- cess research were conducted by counseling psycholo- gists, for example, Edward Bordin, Charles Gelso, Leslie Greenberg, Adam Horvath, Clara Hill, Laura Rice, and Stanley Strong. Returning to the two major divides, regarding the first, we would argue that the increasing dominance of CBT, while derived in part from the early body of research (Chambless et al., 1996) examining and sup- porting its efficacy, is not optimal for the continued
- 54. development of psychotherapy specifically, and clinical psychology more generally. In particular, we suggest that it is highly limiting to have the field dominated by any single theory of change. If CBT were the only effective treatment, this would not be problematic. But converging evidence indicates that CBT is not in fact the only effective treatment, as demonstrated by the Dodo verdict; the fact that, typically, only a small per- centage of outcome variance is accounted for by treat- ment approach (Wampold, 2001); the demonstration of therapist effects and especially (as discussed shortly) the current research evidence that a number of treatments from other theoretical approaches are also efficacious, especially for the treatment for depression (APA Task Force on Psychological Interventions’ 2012 list, http:// www.div12.org/PsychologicalTreatments/disor- ders.html). We suggest that an impartial reading of the psychotherapy efficacy literature would not inevitably
- 55. lead to such a narrow focus on a single theoretical ori- entation. We also suggest that such a narrow focus is very unlikely to encourage and facilitate the research that is sorely needed on other treatment orientations. The evolution of theory, research, and practice requires a diversity of ideas and perspectives, and, as Pauling noted, “lots” of them. Indeed, our current major theoretical perspectives evolved from a combina- tion of mutually enriching, sometimes competing, per- spectives. For CBT, these have included behavioral, psychodynamic, personal construct, social learning, and other perspectives. Messer (2004), in a discussion of “assimilative integration” (i.e., incorporation of tech- niques from other types of treatment into one’s “home” therapy), cited Keane and Barlow’s (2002) observation that Freud and Janet most influenced the use of exposure and anxiety management—now con- sidered central features of CBT—in the treatment for PTSD. More recently, we have seen the experiential
- 56. tradition influencing the evolution of CBT in its new emphasis on affective experience, and the meditative tradition helping to shape Dialectical Behavior Therapy (Linehan,1993) and variations of cognitive-behavioral treatments for generalized anxiety disorder (Roemer, Erisman, & Orsillo, 2008). Additionally, integrative approaches to treating addictions and associated mental health issues, such as motivational interviewing, draw heavily on the client-centered model of therapeutic practice (Angus & Kagan, 2009). Why is the current dominance of a single theoretical perspective potentially problematic? A generation of students trained to think from only one perspective will become theorists, teachers, researchers, and practitio- ners whose creativity, intellectual flexibility, and ability to create new treatments for changing times, troubles, and client populations are likely to be diminished. Further, a generation of students trained (implicitly or
- 57. explicitly) to trust in only one perspective will become a generation that is less willing to be open to different ideas and most importantly, less able to meet the emerging mental health needs of the future. CLINICAL PSYCHOLOGY: SCIENCE AND PRACTICE � V19 N4, DECEMBER 2012 368 John Stuart Mill, a strong advocate of empirical methods in scientific procedure in the 19th century and a philosophical progenitor of behaviorism, argued that a plurality of views is needed in science (Cohen, 1961). Mill’s reasons are as appropriate for training in clinical and counseling psychology as they are for sci- entific advancement, including the fact that a problem- atic view may contain some portion of the truth. Moreover, as the prevailing view is never the whole truth, it is only by collision with contrary opinions that the remainder of the truth has a chance of being recog-
- 58. nized. One point of view that is wholly true, but not subjected to challenge, will be held as a prejudice rather than derived from a rational basis, and someone holding a particular point of view without considering alternative perspectives will not really understand the meaning of the view he or she holds. Citing Mill and framing this argument in a positive form, Safran and Messer (1997) argued that science and practice flourish in an atmosphere of confronting and discussing differ- ence, noting that “to the extent that confronting alter- nate therapeutic paradigms and techniques flips us into a ‘world-revising mode’ … there is the possibility of its leading to a dialogue which can truly deepen our understanding of the human change process” (1997, p. 142). In the clinical realm as well, there are atten- dant implications for the ways in which we think philosophically about human nature and human change. It has been argued that exposing psychology students to different theories and visions of reality
- 59. (Messer & Winokur, 1984) enriches their understand- ing of clients and ways to treat them, including the possibility of shifting from one perspective to another, thereby encompassing more of the complexity of human behavior (Messer, 2006). Paradoxically, having both understanding of and competence with two or more treatment orientations may help clinicians use particular treatment protocols with greater fidelity, when that is their goal. There is mounting evidence that the actual therapeutic interventions of clinicians who believe they are follow- ing manualized treatment protocols often do not accu- rately reflect the core treatment principles of that approach (Shoham, 2011). A proposed remedy, training students to understand the difference between going “off-manual” versus practicing “flexibility within fidelity” (Kendall, Gosch, Furr, & Sood, 2008; Sho- ham, 2011), requires a deep understanding of what is
- 60. and what is not a prototypical intervention in the approach at hand. And the latter, we suggest, is facili- tated by knowing more than one therapeutic approach well because the distinguishing features between cate- gories of interventions help define them. For example, students who truly understand interpretation but who are following a CBT protocol and attempting to frame cognitive restructuring interventions will be more likely to do so with integrity because they understand the differences between these similar yet distinct con- structs at a core level. Finally, we are concerned that the trend shown in these data is likely to beget more of the same over time. The programs most likely to produce our future academic clinical psychologists—comprehensive Ph.D. programs, perhaps especially those designated as clinical science programs—are the ones with the narrowest range of orientations. Not only will this trend limit the vision and sources of ideas for current students, but also
- 61. their students will be even less likely to have professors and clinical supervisors who represent other orienta- tions, and consequently less likely to have research mentors who are engaged in serious research on psy- chotherapy from other orientations. We hasten to note that there is no implied criticism here of the core emphasis of clinical science training programs on the need for data regarding the development and validation of treatment approaches. In fact, one of our goals in this commentary is to emphasize and support the asser- tion that any treatment model worth learning must have compelling data that support its efficacy and effec- tiveness (and in fact, as noted earlier, a range of treat- ment approaches do). Rather, the concern is that we may inadvertently be training a generation of students who equate a particular orientation with “good sci- ence” and, by implication, other orientations for which compelling data in fact exist, with “bad science” or
- 62. “no science.” Finally, inasmuch as the growth and development of treatments is facilitated by ongoing exchanges between researchers and practicing clinicians, these divides are dangerous. There is currently considerable distance between the kinds of treatments that practitioners know and use, on the one hand, and the type of THEORETICAL ORIENTATIONS � HEATHERINGTON ET AL. 369 treatment that has come to dominate the research- based treatment development landscape, that is, CBT, on the other. A 2008 APA survey of 5,051 certified Psychology Health Service Providers in the United States revealed the following “primary theoretical orientations,” in descending order: cognitive behavioral (38.9%), psychodynamic/psychoanalytic (15.6%), inte- grative (14.6%), “other,” which was primarily “eclec-
- 63. tic” (6.1%), cognitive (5.1%), humanistic/existential (4.1%), behavioral (2.9%), systems (2.8%), and less than 2% each of biological, developmental, and family (APA, 2008, http://www.apa.org/workforce/publications/ 08-hsp/index.aspx). Yet, feedback about the clinical realities of imple- menting treatments as well as (ideally) the input of practitioners into treatment development at early stages is critical. A laudable collaborative project between APA’s Division 12 (Clinical Psychology) and Division 29 (Psychotherapy) solicited clinicians’ feedback about their experiences using various cognitive-behavioral approaches for social phobia, generalized anxiety disor- der, and panic (Goldfried, 2010, 2011). This kind of exchange advances intelligent development and refine- ments of our treatments, but it will be less and less likely to happen among, for example, family therapy, psychodynamic, and experiential researchers and practi-
- 64. tioners, given the shrinking numbers of academics ask- ing such questions from these perspectives. LIMITATIONS AND POSSIBLE COUNTERARGUMENTS There are some limitations in the data themselves. Only allegiances to the categories of therapeutic orien- tation included by the Insider’s Guide were assessed; also, objections may be raised to the ways in which the approaches are categorized in that book, for example, separating behavioral and cognitive behavioral, and cat- egorizing all psychodynamic approaches as one. Other orientations (e.g., Interpersonal Therapy [IPT], group, eclectic) are missing altogether. An “integrative” choice would have been particularly relevant to the current questions. As it is not included in the Insider’s Guide, we have no way of knowing whether faculty “orienta- tion” refers to an orientation with regard to one’s clini- cal practice (and indeed, how many faculty are engaged in active clinical practice), personal theoretical prefer-
- 65. ence, research domain, or some combination. Further, the focus of these categories on treatment orientations does not capture allegiance to training orientations that focus on aspects of the therapeutic relationship, which transcend treatment type, but which are also critically important not only for treatment outcome but also for theory development and research (Norcross, 2011). On the other hand, we note that our sample itself is broader and more representative of psychologists cur- rently engaged in training than other surveys of theo- retical orientation, for example, surveys restricted to members of APA’s Division 12 (Clinical Psychology; Norcross, Karpiak, & Santoro, 2005). The data also cannot reveal how the current state of affairs applies to the actual coursework and practicum training offered within the various types of training pro- grams, nor do the percentages include part-time and adjunct faculty who are hired to teach practical and who
- 66. are sometimes involved in supervising theses and disser- tations at Psy.D. and professional school programs, and thus have some influence on doctoral students’ outlooks. We would argue, however, that the impact of their research mentorship may not be as strong as that of core faculty, who are engaged in research and predominantly shape the intellectual ethos of the program. In the spirit of the Popper quote, a counterargument to ours may be mounted, namely, that the evolution we described is precisely what is best for the field. The strongest stance would be that it is no longer accept- able to use—or to train students to use—psychological treatments that have not been empirically supported as efficacious for specific psychological disorders in rigor- ous randomized clinical trial research. On the other end, there are stances that allow for evidence-based practice and training (Levant & Hasan, 2008) that in addition to basing practice on findings from random- ized clinical trials, more explicitly recognize the role of
- 67. clinical expertise, client values and preferences, and other forms of research evidence (Messer, 2004). There are a variety of opinions about the standards by which the acceptability of evidence for a treatment should be decided. We will not hash out the empirically sup- ported treatments debate here as it has been thoroughly discussed in the literature, but we acknowledge that individuals’ and programs’ stances on what constitutes acceptable evidence of treatment effectiveness/efficacy are a key factor in training policies. CLINICAL PSYCHOLOGY: SCIENCE AND PRACTICE � V19 N4, DECEMBER 2012 370 We agree that training students in a diversity of poor or wholly untested treatments for the sake of hav- ing a variety of options makes no sense and that dis- credited theories and treatments (cf. Castonguay, 2010; Lilienfeld, 2007), as well as those for which no one
- 68. seems to be willing or able to mount research programs to evaluate, should be “eliminated as unfit.” But we are a long way from the claim that only cognitive-behav- ioral treatments are empirically supported. As Messer (2004) noted, the literature also reveals a number of what Wampold (2001) defined as “bonafide” therapies: those with a firm theoretical base, an extensive practice history, and a research foundation, even if the treat- ment does not meet the “empirically supported” crite- ria as defined by the Task Force (Wampold, Minami, Baskin, & Tierney, 2002; Wampold et al., 1997). Indeed, as noted earlier, the updated APA Division 12 list of research-supported treatments for depression now goes far beyond the narrow range of treatment approaches originally identified and includes 12 differ- ent empirically supported treatments for depression that are based on humanistic, psychodynamic, interpersonal, and cognitive therapy models (http://www.div12.org/
- 69. PsychologicalTreatments/disorders.html). Yet, the increas- ing lack of opportunity for serious graduate study and research on the full range of evidence-based approaches risks creating a situation in which their development will fall increasingly behind, widening these divides. POSSIBLE SOLUTIONS AND FUTURE DIRECTIONS First, preparing students to think in an integrative man- ner may help. It has been demonstrated that the funda- mental tenets of one theory also explain client change from other theoretical perspectives. Consider operant conditioning, a hallmark of CBT, which Castonguay, Reid, Halperin, and Goldfried (2003) found to occur in psychodynamic as well as humanistic therapies. Contrariwise, there are features of CBT that are bor- rowed, knowingly or not, from psychodynamic therapy and that are correlated with change in CBT (Shedler, 2010). The psychotherapy integrationist movement has a long history, which includes Dollard and Miller’s
- 70. (1950) comparative analysis of behaviorism and psychoanalysis, Frank’s (1961) description of curative factors in healing across cultures, and Lazarus’s (1967) technical eclecticism and multimodal therapy. The growing trend toward integration came from major theorists who recognized the complexity of the change process and the shortcomings of many unimodal theo- ries. In his 2010 presidential address to the Society for Psychotherapy Research, Castonguay predicted that psychotherapy integration will continue to grow and that the four major systems of therapy will be improved based on research that emphasizes common and contextual factors with diverse client populations. According to him, as we narrow the division between research and clinical practice, integrative psychotherapy is likely to become the gold standard, even if it is not superior to a “pure form” approach. In our data set, there were a few programs that were clearly integra-
- 71. tionist evidenced by both a variety of orientations rep- resented and a total number of orientations listed that was well over 100%. Furthermore, a substantial body of efficacy research indicates that successful treatment is accounted for by individual client differences, individ- ual therapist effects, and common factors (expectancy, alliance, etc.) more so than by techniques specific to any particular theoretical orientation (Wampold, 2001). Thus, truly integrative thinking requires training in these research and theoretical bases as well. Second, the training of top-notch future psychother- apists, psychotherapy theorists, and psychotherapy researchers needs to include an understanding of the latest clinical science in related domains of knowledge such as developmental psychopathology and affective neuroscience. For example, attachment, emotion regu- lation, autobiographical memory specificity, and per- ceptual-cognitive biases, among many other topics, are
- 72. highly relevant to therapy; not only will this under- standing enrich the pool of ideas that inform the study of change process mechanisms, but also it will enhance entry-level clinicians’ ability to think broadly and deeply about how and when to use the tools they have. It is erroneous to assume that one orientation is more compatible with basic science than another, the current data notwithstanding. The challenge, of course, is to be true to the intent of training models—to actu- ally expose students to science, teach them how to understand it (and in some cases, how to engage in it), and most importantly, help them to integrate emerging findings in behavioral and clinical science into their practices. THEORETICAL ORIENTATIONS � HEATHERINGTON ET AL. 371 Third, we suggest that monocultures, or near mono- cultures, tend to reproduce themselves in both subtle
- 73. and less subtle ways without deliberate attention to intellectual diversity. The chance to talk with col- leagues from other theoretical orientations as well as from related disciplines is affected by program infra- structure, from the seemingly mundane (office and lab- oratory placements, research group assignments, habits of colloquia invitations and attendance) to the less mundane (faculty hiring and graduate student admission practices, tenure and promotion pressures that foster not straying too far from colleagues’ beliefs or prevail- ing department culture). Professional conferences, with a few exceptions (Society for Psychotherapy Integra- tion, Society for Psychotherapy Research), have become increasingly balkanized, top-ranked doctoral programs tend to admit students whose prior training and attitudes about theoretical orientation are fairly set and mirror that of their potential advisor, and grant pressures (which currently favor the predominant treat-
- 74. ment approach) help keep students fairly narrowly focused from the time they enter their doctoral pro- grams. Our field needs to think collectively about the implications of such practices. Finally, it bears repeating that advocates of promising treatment approaches that are not widely available for training at present and that do still require stronger empirical evidence need to continue their research efforts and to be better sup- ported in doing so. It is interesting and hopeful in this regard that those doctoral programs in comprehensive universities not designated as clinical science programs, and the doctoral programs in counseling psychology, had the highest mean percentages of multiple orienta- tions claimed, 129% and 114%, respectively. It will be interesting to see whether or not future psy- chotherapy training continues to be organized around broad umbrella “orientations” or organized more around some other features of treatments. We note, for
- 75. example, that CBT now represents a highly diverse cate- gory of evidence-based protocols (EBPs), which are quite different from each other in underlying theories of change (e.g., exposure in Prolonged Exposure [PE], cognitive restructuring in Cognitive Processing Therapy [CPT]), structures (90-min sessions in PE, 60-min ses- sions in CPT), and techniques/procedures (in-session, repeated imaginal exposures in PE, use of written narra- tives in CPT). In fact, the United States Department of Veterans Affairs (VA) purports to provide training and dissemination of specific EBPs for clinicians providing mental health services to veterans (Karlin et al. 2010). The VA’s list of these includes the following: CBT for depression, Acceptance and Commitment Therapy (ACT) for depression, IPT for depression, CPT for PTSD, PE for PTSD, Social Skills Training (SST) for severe mental illness, Integrative Behavioral Couple Therapy (IBCT), and Family Psychoeducation.
- 76. Should graduate psychotherapy training programs aspire to training models that de-emphasize a focus on particular theoretical orientations and focus more than at present on training in a broad range of evidence- based protocols? On the one hand, it would be a way for students to acquire knowledge earlier in a range of efficacious treatments so that internship and postdoc- toral psychotherapy training could be organized around providing more advanced training and supervision. (Currently, many internship and postdoctoral training sites can only provide introductory exposure to evi- dence-based protocols from approaches other than CBT, due to students’ very limited [if any] exposure to these approaches during graduate training.) Further, it might be expected that with experience and supervi- sion, trainees in EBPs naturally evolve toward integra- tion and adaptation of EBPs according to the unique characteristics of individual patients. On the other
- 77. hand, it could be argued that this kind of training strat- egy, especially at the graduate (vs. internship or extern- ship) level, would be atheoretical, too narrow and too focused on specific protocols. Rather, students should be trained in the broader theoretical outlooks and non- specific relationship skills, and only then in the specific EBPs, which will lead naturally to an integrative approach informed by a deeper understanding. In another vein, Follette and Beitz (2003) offer some sensible suggestions for creating a curriculum that teaches students to think in a broad and rigorous scien- tific manner about empirically supported treatments. Specifically, these suggestions call for more attention to mechanisms of psychotherapeutic change, which is by definition a multitheoretical or even pantheoretical enterprise, at least. In addition, programs seeking to build strength in training for more than one orientation should “put their best foot forward” by highlighting
- 78. CLINICAL PSYCHOLOGY: SCIENCE AND PRACTICE � V19 N4, DECEMBER 2012 372 the available data, exposing students to the theoretical and empirical base that justifies training in a particular orientation. In sum, healthy evolution in our field, as in all fields, requires new ideas that derive from varying per- spectives. As clinical science progresses, this kind of flexibility, which transcends singular allegiances to one theoretical orientation versus another, will become increasingly important in the development of theory, research, and practice. ACKNOWLEDGMENTS We gratefully acknowledge the able research assistance of Laura Christianson and Joshua Wilson, and very helpful com- ments from Marlene Sandstrom, Catherine B. Stroud, and an anonymous reviewer. NOTES
- 79. 1. These are programs that have been determined to meet the criteria outlined by the Academy of Psychological Clini- cal Science and thus designated by that body as “clinical sci- ence” programs. See http://acadpsychclinicalscience.org/ members. 2. The raw data, including a list of programs in each cate- gory, are available upon request. REFERENCES Academy of Psychological Clinical Science. (2012). Member programs. Retrieved June 11, 2011, from http:// acadpsychclinicalscience.org/members. American Psychological Association. (2008). Survey of psychologist-members. Retrieved June 1, 2011, from http://www.apa.org/workforce/publications/08-hsp/index. aspx American Psychological Association. (2009). Graduate study in clinical psychology. Washington, DC: Author. American Psychological Association. (2011). Accredited
- 80. programs in clinical psychology. Retrieved June 1, 2011, from http://apa.org/ed/accreditation/programs/index.aspx American Psychological Association Task Force on Psychological Interventions. (2012). Division 12 Society of Clinical Psychology. Retrieved June 15, 2012, from http:// www.div12.org/PsychologicalTreatments/disorders.html Angus, L., & Kagan, F. (2009). Therapist empathy and client anxiety reduction in motivational interviewing: “She carries with me, the experience.” Journal of Clinical Psychology: In Session, 65, 1156–1167. Baker, T. D., McFall, R. M., & Shoham, V. (2009). Current status and future prospects of clinical psychology: Toward a scientifically principled approach to mental and behavioral health care. Psychological Science in the Public Interest, 9, 67–103. Bray, J. H. (2011). Training for the future of clinical psychology practice. Training and Education in Professional Psychology, 5, 69–72.
- 81. Calhoun, K. S., Moras, K., Pilkonis, P., & Rehm, L. P. (1998). Empirically supported treatments: Implications for training. Journal of Consulting and Clinical Psychology, 66, 151–162. Castonguay, L. G. (2010). A promising dawn: Integrative connections in psychotherapy. Presidential address, annual conference of the Society for Psychotherapy Research, Monterey, CA. Castonguay, L. G., Reid, J. J., Halperin, G. S., & Goldfried, M. R. (2003). Psychotherapy integration. In G. Stricker & T. A. Widiger (Eds.), Comprehensive handbook of psychology, Vol. 8: Clinical Psychology (pp. 327–345). New York: Wiley. Chambless, D. L., Sanderson, W. C., Shoham, V., Bennett Johnson, S., Pope, K. S., Crits-Christoph, P., et al. (1996). An update on empirically validated therapies. The Clinical Psychologist, 49, 5–18. Cohen, M. (Ed.). (1961). The philosophy of John Stuart Mill. New York: Modern Library. Davison, G. C. (1998). Being bolder with the Boulder
- 82. model: The challenge of education and training in empirically supported treatments. Journal of Consulting and Clinical Psychology, 66, 163–167. Dollard, J., & Miller, N. E. (1950). Personality and psychotherapy. New York: McGraw-Hill. Eby, M. D., Chin, J. L., Rollock, D., Schwartz, J. P., & Worrell, F. C. (2011). Professional psychology training in the era of a thousand flowers: Dilemmas and challenges for the future. Training and Education in Professional Psychology, 5, 57–68. Egan, G. (2007). The skilled helper: A problem-management and opportunity-development approach to helping (8th ed.). Belmont, CA: Brooks/Cole. Follette, W. C., & Beitz, K. (2003). Adding a more rigorous scientific agenda to the empirically supported treatment movement. Behavior Modification, 27, 369–386. Frank, J. (1961). Persuasion and healing. Baltimore: Johns Hopkins University Press.
- 83. Friedlander, M. L., Pieterse, A. L., & Lambert, J. E. (2012). The evolution of theory in counseling psychology. In N. Fouad, L. Subich, & J. Carter (Eds.), APA handbook of counseling psychology (pp. 31–58). Washington, DC: American Psychological Association. THEORETICAL ORIENTATIONS � HEATHERINGTON ET AL. 373 Gelso, C. J., & Fretz, B. (1992). Counseling psychology. New York: Harcourt Brace Jovanovich. Goldfried, M. R. (2010). Clinicians’ experiences in using an empirically supported treatment (EST) for panic disorder: Results of a survey. Retrieved June 15, 2012, from http://www.div12.org Goldfried, M. R. (2011). Generating research questions from clinical experience: Therapists’ experiences using CBT for Panic Disorder. The Behavior Therapist, 34, 57–62. Hill, C. E. (2004). Helping skills: Facilitating exploration, insight,
- 84. and action (2nd ed.). Washington, DC: American Psychological Association. Ivey, A. E., & Ivey, M. B. (2007). Intentional interviewing and counseling: Facilitating client development in a multicultural society (6th ed.). Pacific Grove, CA: Brooks/Cole. Karlin, B. E., Ruzek, J. I., Chard, K. M., Eftekhari, A., Monson, C. M., Hembree, E. A., et al. (2010). Dissemination of evidence-based psychological treatments for posttraumatic stress disorder in the Veterans Health Administration. Journal of Traumatic Stress, 23, 663–673. Keane, T. M., & Barlow, D. H. (2002). Posttraumatic stress disorder. In D. H. Barlow (Ed.), Anxiety and its disorders (2nd ed., pp. 418–453). New York: Guilford. Kendall, P. C., Gosch, E., Furr, J. M., & Sood, E. (2008). Flexibility within fidelity. Journal of the American Academy of Child and Adolescent Psychiatry, 47, 987–993. Lazarus, A. A. (1967). In support of technical eclecticism. Psychological Reports, 21, 415–416.
- 85. Levant, R. F., & Hasan, N. T. (2008). Evidence-based practice in psychology. Professional Psychology: Research and Practice, 39, 658–662. Lilienfeld, S. (2007). Psychological treatments that cause harm. Perspectives on Psychological Science, 2, 53–69. Linehan, M. M. (1993). Cognitive-behavioral treatment of borderline personality disorder. New York: Guilford. McFall, R. M. (2007). On psychological clinical science. In T. A. Treat, R. R. Bootzin, & T. B. Baker (Eds.), Psychological clinical science: Papers in honor of Richard M. McFall (pp. 363–396). New York: Psychology Press. Messer, S. B. (2004). Evidence-based practice: Beyond empircially supported treatments. Professional Psychology: Research and Practice, 35, 580–588. Messer, S. B. (2006). Psychotherapy integration based on contrasting visions of reality. In G. Stricker, & J. Gold (Eds.), Casebook of psychotherapy integration (pp. 281–291). Washington, DC: American Psychological Association Press.
- 86. Messer, S. B., & Winokur, M. (1984). Ways of knowing and visions of reality in psychoanalytic therapy and behavior therapy. In H. Arkowitz, & S. B. Messer (Eds.), Psychoanalytic therapy and behavior therapy: Is integration possible? (pp. 63–100). New York: Plenum. Munsey, C. (2011). The internship match crisis continues. Monitor on Psychology, 42(4), 12–13. Norcross, J. C. (Ed.). (2011). Psychotherapy relationships that work: Evidence-based practice (2nd ed.). New York: Oxford University Press. Norcross, J. C., Karpiak, C. P., & Santoro, S. O. (2005). Clinical psychologists across the years: The Division of Clinical Psychology from 1960 to 2003. Journal of Clinical Psychology, 61, 1467–1483. Ridley, C. R., Kelly, S. M., & Mollen, D. (2011). Beyond microskills: Toward a model of counseling competence. The Counseling Psychologist, 39, 825–864.
- 87. Roemer,L.,Erisman, S.M.,&Orsillo,S.M.(2008).Mindfulness and acceptance-based treatments for anxiety disorders. In M. M. Antony, & M. B. Stein (Eds.), Handbook of anxiety and the anxiety disorders (pp. 476–487). NewYork: Oxford University Press. Safran, J., & Messer, S. B. (1997). Psychotherapy integration: A postmodern critique. Clinical Psychology: Science and Practice, 4, 140–152. Sayette, M. A., Mayne, T. J., & Norcross, J. C. (2010). Insider’s Guide to Graduate Programs in Clinical and Counseling Psychology. New York: Guilford. Sayette, M. A., Norcross, J. C., & Dimoff, J. D. (2011). The heterogeneity of clinical psychology Ph.D. programs and the distinctiveness of APCS programs. Clinical Psychology: Science and Practice, 18, 4–11. Shedler, J. (2010). The efficacy of psychodynamic psychotherapy. American Psychologist, 65, 98–109. Shoham, V. (2011). Treatment fidelity: The elusive independent
- 88. variable. Paper presented at the North American Society for Psychotherapy Research conference, Banff, Alberta. Vasquez, M. J. T. (2011). The internship crisis: Strategies and solutions. Monitor on Psychology, 42(4), 5. Wampold, B. E. (2001). The great psychotherapy debate. New York: Lawrence Erlbaum. Wampold, B. E., Minami, T., Baskin, T. W., & Tierney, S. C. (2002). A meta-(re) analysis of the effects of cognitive therapy versus ‘other therapies’ for depression. Journal of Affective Disorders, 68, 159–165. Wampold, B. E., Mondin, G. W., Moody, M., Stich, F., Benson, K., & Ahn, H. (1997). A meta-analysis of outcome studies comparing bona fide psychotherapies: Empirically, ‘all must have prizes’. Psychological Bulletin, 122, 203–215. Received February 5, 2012; accepted October 2, 2012. CLINICAL PSYCHOLOGY: SCIENCE AND PRACTICE � V19 N4, DECEMBER 2012 374 Copyright of Clinical Psychology: Science & Practice is the
- 89. property of Wiley-Blackwell and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.