Seminar tos THORACIC OUTLET SYNDROME
•Download as PPT, PDF•
58 likes•4,838 views

Thoracic outlet syndrome is caused by compression of the neurovascular structures in the thoracic outlet. It can be caused by abnormalities such as cervical ribs or anomalies of the scalene muscles. Symptoms include pain, numbness, and weakness in the arm. Diagnosis involves clinical exams like Adson's test and imaging tests. Treatment begins with non-operative measures like posture improvement and physical therapy. Surgery to remove compressive structures may be needed if symptoms persist. Recurrence after surgery can occur if all abnormal structures were not removed and may require re-operation using the posterior thoracoplasty approach along with neurolysis and sympathectomy.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Seminar tos THORACIC OUTLET SYNDROME
Similar to Seminar tos THORACIC OUTLET SYNDROME (20)
More from Dr. Vinita
More from Dr. Vinita (14)
Recently uploaded
Recently uploaded (20)
Seminar tos THORACIC OUTLET SYNDROME
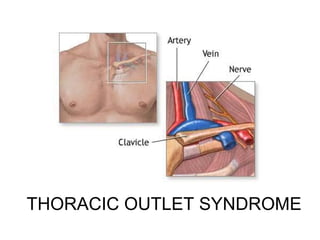
- 2. Thoracic outlet syndrome (TOS)- a collection of symptoms brought about by abnormal compression of the neurovascular bundle by bony, ligamentous or muscular obstacles in the narrow space between clavicle and 1st rib.
- 3. ANATOMY Interscalene triangle − Med : 1st rib − Ant : clavicle, scaleneus anterior − Post : scaleneus medius Costoclavicular space − Med : 1st rib − Ant : clavicle − Post : scaleneus anterior − Lat : costoclavicular ligament, subclavius muscle Subcoracoid tunnel compressed by pectoralis minor tendon, head of humerus or coracoid process.
- 8. Causes Cervical rib Long C7 transverse process Anomalous insertion of scalene muscles Scalene muscle hypertrophy Scaleneus minimus Abnormal bands, ligaments Fracture clavicle/ 1st rib Exostosis Tumours Brachial plexus trauma / diseases
- 9. Cervical rib A cervical rib is a supernumerary (or extra) rib which arises from the seventh cervical vertebra. Sometimes known as "neck ribs" Congenital abnormality located above the normal first rib. A cervical rib is present in only about (0.2%) of people. Half unilateral, common in right side. Usually asymptomatic
- 10. Types : 1) Completely bony 2) Completely fibrous 3) Combined 4) Bony swelling
- 11. Type 3 is most common. Type 3 – a band stretching from C7 vertebra to Scalene tubercle on 1st rib. It elevates the neurovascular bundle compressing it in the interscalene triangle.
- 13. Cervical rib
- 14. Cervical rib
- 15. Clinical features Most commonly seen in middle aged women Usually due to neural compromise. Interscalene triangle Artery , Nerves Scaleneus anticus syndrome Costoclavicular space Vein Edens syndrome Subcoracoid area Artery, Vein , Nerves Hyperabduction syndrome
- 19. Arterial compromise Fatigue Weakness Coldness Upper limb claudication Thrombosis Paraesthesia Gangrene Raynaud's phenomenon due to thrombosis with distal embolisation
- 21. Venous compromise Edema Venous distension Collateral formation Cyanosis Paget-Schroetter syndrome – effort thrombosis − "Effort" axillary-subclavian vein thrombosis (Paget- Schroetter syndrome) is an uncommon deep venous thrombosis due to repetitive activity of the upper limbs.
- 22. Neural compromise Paraesthesia Pain in shoulder, arm, forearm and fingers Occipital headache – referred from tight scalene muscles Weakness of forearm, hand.
- 23. Clinical tests
- 24. Roos Test Hold both arms in surrendering position (90°overhead with shoulders in external rotation) – reproduction of symptoms within 1 minute . Arm collapses if continued. modified Roos test / Elevated Arm Stress Test(EAST)– same as above. Symptoms precipitated by opening and closing fists continuously.
- 25. Elevated arms stress test
- 26. Adson's (Scalene) Test Radial pulse diminishes and disappears on turning chin to same side. Decreases space between scaleneus anterior and medius .
- 27. Adsons test
- 28. Halsted's costoclavicular compression test 45° abduction and extension of arm with downward pressure on shoulders –neck turned to opposite side- reproduce symptoms
- 29. Exaggerated military position Patient shrugs shoulders with deep inhalation while drawing the shoulders backward in an exaggerated military position – radial pulse diminishes.
- 31. Wright's hyperabduction test Arm hyperabducted to 180°-diminishing radial pulse. Neurovascular structures compressed in subcoracoid region by pectoralis minor tendon, head of humerus or coracoid process.
- 33. Tinel sign – in supra and infraclavicular region Phalens sign – in carpel tunnel syndrome (CTS)
- 34. Differential diagnoses Carpel tunnel syndrome Spinal canal tumors Shoulder myositis Angina pectoris Raynaud's disease Ulnar nerve compression - epicondylitis
- 35. Investigations Chest x ray, cervical spine x ray MRI, cervical myelography − r/o narrowing of intrevertebral foramen, disc compression. Doppler , vascular imaging(angiogram/venogram) − r/o aneurism, thrombosis Nerve conduction study, electromyography − confirm neurogenic TOS, localise the area of compression- r/o CTS
- 36. Double crush syndrome – TOS with other peripheral sites of nerve compression(CTS)
- 37. Treatment
- 38. Non operative treatment Posture improving exercises. Breathing exercises. Avoid aggravating activities. Avoid repetitive upper extremity mechanical work and muscular trauma. Analgesics,muscle relaxants, antidepressants. Physiotherapy .
- 39. Surgical treatment Indications: Symptoms persists with non operative treatment. Associated vascular compression. Progression of neurological symptoms. Nerve conduction velocity < 60m/s
- 40. Trans cervical or trans axillary(Roos) resection of 1st rib often with release of scalene muscles. Extraperiosteal excision of Cervical rib(to prevent its regeneration) .Often a cervical sympathectomy is also needed.
- 41. Roos approach
- 42. 42 F. RECURRENT THORACIC OUTLET SYNDROME 1. 10% of surgically treated patients have shoulder, arm or hands pain and pareathesia. Most patients can be relieved with physiotherapy and muscle relaxant. 2. In 1.6% of patients, symptoms exacerbate and persist. 3. Most recurrences occur in 3 months postoperatively.
- 43. 43 F. RECURRENT THORACIC OUTLET SYNDROME 4. Pseudorecurrence (1) A 2nd rib was mistakenly resected for a 1st rib (2) A 1st rib was resected but a cerical rib was left. (3) A cervical rib was resected but an abnormal 1st rib was left. (4) A 2nd rib was resected but a rudimentary 1st rib was left.
- 44. 44 F. RECURRENT THORACIC OUTLET SYNDROME 5. True recurrence The 1st rib was not resected completely. 6. All patients with recurrence after 1st rib resection should undergo physiotherapy. If symptoms persist and UNCV is still low then re-operation is indicated. 7. Re-operation is always done through the posterior thoracoplasty approach.
- 45. 45 F. RECURRENT THORACIC OUTLET SYNDROME 8. The anterior or supraclavicular approach is not adequate for re-operation. 9. The basic elements for re-operation are (1) resection of recurrent or persistent bony remnants (2) neurolysis of the brachial plexus or nerve roots (3) dorsal sympathectomy of T1, T2, T3 ganglia
- 46. 46 F. RECURRENT THORACIC OUTLET SYNDROME 10. The technique includes a high thora- coplasty incision, extending 3 cm above the angle of the scapula, halfway between the angle of the scapula and spinous processes, and caudate 5 cm from the angle of scapula. 11. The trapezius and rhomboid muscles are divided..
- 47. 47 F. RECURRENT THORACIC OUTLET SYNDROME 12. The scapula is retracted by incision of the LD muscle over the 4th rib. 13. The posterior superior serratus muscle was divided and sacrospinalis muscle is retracted medially. 14. The 1st and cervical rib must be resected, if present subperiosteally. 15. The regenerated periosteum is extirpated.
- 48. 48 F. RECURRENT THORACIC OUTLET SYNDROME 16. If excessive scar is present the it is necessary to perform sympathectomy initially. This involves resection of a 1- inch segment of 2nd rib posteriorly to locate the sympathetic ganglia. 17. Neurolysis is performed using a nerve stimulator but not into the sheath.
- 49. 49 F. RECURRENT THORACIC OUTLET SYNDROME 18. A J-P drain is left in the area of brachial plexus. Depo-Medral, 80 mg, is left in the area of brachial plexus. 19. The arm is kept in sling to be used gently for 3 months. 20. When the problem is vascular, involving false or mycotic aneurysms, bypass graft is interposed. The saphenous vein is usually used.
- 50. 50 F. RECURRENT THORACIC OUTLET SYNDROME 21. 7% of patients underwent 2nd re-operation for rescarring. No death occurred. Only one patient had infection and needed drainage.
- 51. Thank you....