
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Autologous condrocyte implantation
Similar to Autologous condrocyte implantation (20)
Recently uploaded
Recently uploaded (20)
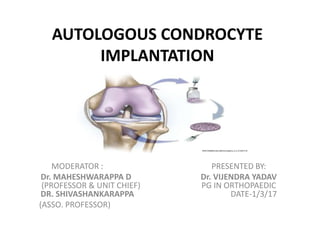
Autologous condrocyte implantation
- 1. AUTOLOGOUS CONDROCYTE IMPLANTATION MODERATOR : PRESENTED BY: Dr. MAHESHWARAPPA D Dr. VIJENDRA YADAV (PROFESSOR & UNIT CHIEF) PG IN ORTHOPAEDIC DR. SHIVASHANKARAPPA DATE-1/3/17 (ASSO. PROFESSOR)
- 2. INTRODUCTION • Autologous chondrocyte implantation (ACI) for the treatment of articular cartilage lesions of the knee joint provides successful and durable long- term outcomes. • The treatment of symptomatic cartilage defect is a challenging problem as injuries of the articular cartilage do not heal spontaneously.
- 3. • To address this, ACI was first performed in Gothenburg, Sweden, in 1987 by Lars Peterson, and his first cohort of cases with second-look biopsies was reported in 1994. • The first-generation ACI were performed with an autologous periosteal flap from the tibia or femur to cover the defect and seal in the cultured autologous chondrocytes.
- 4. • Second-generation ACI involved the use of a bioabsorbable scaffold carrier for the cells. These scaffolds include a hyaluronan weave (Hyalograft C; Fidia Advanced Biopolymers), collagen scaffolds (MACI; Genzyme Biosurgery) and gels derived from collagen (CaReS; Arthro Kinetics).
- 5. • ACI is a two-stage procedure, beginning with arthroscopic assessment of the chondral injury and biopsy to harvest approximately 200 to 300 mg of cartilage, followed by a commercial enzymatic digestion and cell expansion in monolayer culture with cryopreservation of the cells. The cryopreserved cells are thawed and expanded to the cell population needed for the second- stage open ACI technique.
- 6. GENERAL FEATURES OF CARTILAGE • Cartilage is derived (embryologically) from mesenchyme. • Some mesenchymal cells differentiate into cartilage forming cells or chondroblasts. • Chondroblasts produce the intercellular matrix as well as the collagen fibres that form the intercellular substance of cartilage. • Chondroblasts that become imprisoned within this matrix become chondrocytes. • Some mesenchymal cells that surround the developing cartilage form the perichondrium. • Perichondrium contains cells that are capable of transforming themselves into cartilage cells when required.
- 7. • Cartilage has very limited ability for regeneration (after destruction by injury or disease). Defects in cartilage are usually filled in by fibrous tissue.
- 8. • Cartilage is usually described as an avascular tissue. However, the presence of cartilage canals, through which blood vessels may enter cartilage, is well documented. Each canal contains a small artery surrounded by numerous venules and capillaries. • Cartilage cells receive their nutrition by diffusion from vessels in the perichondrium or in cartilage canals.
- 9. • Growth of cartilage: Newly formed cartilage grows by multiplication of cells throughout its substance. • This kind of growth is called interstitial growth. Interstitial growth, is possible only as long as the matrix is sufficiently pliable to allow movement of cells through it. • As cartilage matures the matrix hardens and the cartilage cells can no longer move widely apart; in other words interstitial growth is no longer possible.
- 10. • At this stage, when a cartilage cell divides the daughter cells remain close together forming cell nests. • Further growth of cartilage now takes place only by addition of new cartilage over the surface of existing cartilage; this kind of growth is called oppositional growth. • It is possible because of the presence of cartilage forming cells in the deeper layers of the perichondrium
- 11. • The articular surface of most synovial joints are lined by hyaline cartilage. • The articular cartilages provide the bone ends with smooth surfaces between which there is very little friction. • They also act as shock absorbers. • Articular cartilages are not covered by perichondrium. • Their surface is kept moist by synovial fluid that also provides nutrition.
- 12. COMPONENTS OF CARTILAGE • Like ordinary connective tissue, cartilage is made up of: • Cells—chondrocytes • Ground substance/matrix • Fibres—collagen fibres
- 13. CARTILAGE CELLS • The cells of cartilage are called chondrocytes. • They lie in spaces (or lacunae) present in the matrix. • At first the cells are small and show the features of metabolically active cells. • The nucleus is euchromatic. • Mitochondria, endoplasmic reticulum (ER) and Golgi complex are prominent. • As the cartilage cells mature they enlarge, often reaching a diameter of 40 um • The nuclei become heterochromatic and organelles become less prominent.
- 14. GROUND SUBSTANCE • The ground substance of cartilage is made up of complex molecules containing proteins and carbohydrates (proteoglycans). • The carbohydrates are chemically glycosaminoglycans (GAG). • They include chondroitin sulphate, keratin sulphate and hyaluronic acid. • The core protein is aggrecan.
- 15. COLLAGEN FIBRES OF CARTILAGE • The collagen fibres present in cartilage are chemically distinct from those in most other tissues. • They are type II collagen. • However, fibrocartilage and the perichondrium, contain the normal type I collagen.
- 16. HYALINE CARTILAGE • Hyaline cartilage is so called because it is transparent (hyalos = glass). • The fibres are arranged so that they resist tensional forces. The ground substance resists compressive forces, while the collagen fibres resist tensional force. • In haematoxylin and eosin stained preparations, the matrix is stained blue and it is basophilic. However, the matrix just under the perichondrium is acidophilic.
- 17. • Towards the centre of a mass of hyaline cartilage the chondrocytes are large and are usually present in groups (of two or more). • The groups are formed by division of a single parent cell. • The cells tend to remain together as the dense matrix prevents their separation. • Groups of cartilage cells are called cell-nests (or isogenous cell groups).
- 18. INDICATIONS AND CONTRAINDICATIONS Indications • Symptomatic focal chondral and osteochondral defects • defect of > 2 cm2 on the femur or patella • Age of 13 to 55 years • Patient's willingness and ability to comply with postoperative rehabilitation • Defects for which other treatments have failed
- 19. Contraindications • More than 50% loss of cartilage thickness (joint space narrowing) • Inflammatory joint disease • Unresolved septic arthritis or treatment of septic arthritis within the previous 12 months. • Metabolic or crystal disorder • Deficient soft-tissue coverage • Patient currently smoking • Obesity (body mass index >35 kg/m2) • Chronic narcotic use • Age >55 years (relative contraindication) • Allergy to collagen.
- 20. Identifying a Carticel Patient Patient Factors: • Younger patients – < age 55 (avg. ~ 35 yr) • Significant impairment: – Compromised daily living activities. – Refractory to treatment • Obesity • Demanding Physical activities • Willing & capable of rehabilitation program
- 21. Joint Factors: • Symptomatic cartilage defects – Moderate to large (> 2cm2 d.= 1.6) – On the distal femur (mfc / lfc ) – Average defect size > 4 cm2 – Either chondral or osteochondral • Relatively healthy joint – – No arthritis • Co-morbidities(meniscal tear, instability or mal-alignment) must be corrected prior or concurrent to implantation.
- 22. Pre-requisite for surgery : • Appropriate biomechanical alignment • Ligamentous stability • Range of motion Not recommended for patients who have : • An unstable knee • Patients sensitive to materials of bovine origins • Allergic to the antibiotic gentamicin • In children • Yet in any joint other than the knee.
- 23. INVESTIGATIONS Wt bearing x-ray • Evidence of joint space narrowing 50% with osteophyte formation, subchondral bony sclerosis or cyst formation eliminates patients from treatment (ie, if bone on bone changes are present)
- 24. MRI • MRI scanning, while helpful for soft-tissue evaluation of meniscal or ligamentous injury as well as assessment of bone bruises and osteonecrosis. • Does not have a high sensitivity and specificity (75% to 93%) for determining the extent of a chondral injury or subtle chondromalacia changes.
- 25. • The gold standard for determining whether a symptomatic patient is a candidate for ACI are normal radiographs, accompanied by an arthroscopic assessment showing focal pathology.
- 26. ARTHROSCOPY • Extent of lesion, Menisci, AP length of lesion. • Quality and thickness of the surrounding articular cartilage will determine whether healthy cartilage will be available for periosteal suturing or a non-contained chondral injury will require suturing through synovium or small drill holes through the bone.
- 27. SURGICAL TECHNIQUES • Uses your own cartilage cells (chondrocytes) to repair the articular cartilage damage in your knee. • When implanted into a cartilage injury, your own cells can form new cartilage; this new cartilage injury is very similar to your original cartilage. • The CARTICEL implantation procedure is called Autologous Chondrocyte Implantation or ACI. • It is a two-step process
- 28. Stage I: Biopsy • The first stage involves an arthroscopic evaluation of the focal chodral lesion to assess containment, depth, and potential bone loss.
- 29. • A biopsy of normal hyaline cartilage is obtained from either the supero-medial or lateral femoral condyle or inner edge of lateral femoral condyle at the intercondylar notch using a curved bone-graft harvesting gouge.
- 30. • The total volume of the biopsy should be approximately 200 to 300 mg .
- 31. • It is better to penetrate to the subchondral bone to ensure that the deep chondrocytes are included in the biopsy. • The biopsy is sent to product labs for processing and cellular expansion. • Biopsy can be stored upto two year.
- 32. Stage II: Implantation • The second stage of the procedure is cell implantation, which takes place between 1 and 24 months following the biopsy. • During this stage arthrotomy done to expose knee and any dead or damaged tissue from the injury removed with curette, leaving only healthy tissue .
- 33. Defect before (A) and after (B) preparation.
- 34. • The periosteal patch is harvested through a 3cm incision on proximal medial tibia.
- 35. • A patch that is at least 2mm larger than the defect is harvested to account for slight shrinkage following detachment. • The patch is then sewn onto the cartilage with the cambium layer facing the defect. • Carticel injects under the patch.
- 36. • After cell implantation, the sutured periosteal patch is sealed with fibrin glue
- 38. In Vitro Human chondrocyte growth Cartilage Biopsies: • The cartilage fragments had 1cm² area in diameter and were transported immediately after harvesting in sterile tubes containing phosphate buffered saline (penicillin/streptomycin and Amphotericin B).
- 39. Chondrocyte Isolation from Cartilage: • A sterile scalpel was used to cut the cartilage into small pieces and transferred to Petri dish. • Sliced cartilages were maintained overnight at 37°C, 5% CO₂ as in ham's F12: DMEM containing fetal bovine serum, ascorbic 100 mg/ml and penicillin/streptomycin 100 u/100 mg/ml to ensure sterility of the specimens prior to enzymes digestion, the time of enzymatic digestion was adapted to the size of tissue fragments. • The prepared cartilage was washed in phosphate buffered saline (PBS) containing antibiotics.
- 40. • The tissue was then incubated in the above growth medium containing trypsin at 37°C, 5% CO₂ for 30 minutes. • Supernatants were discarded and the cartilage was further digested in growth medium containing 0.8 mg/ml collagenase II for 4 hours at 37°C, 5%CO₂. • The digested tissue was then allowed to settle and the supernatant containing the cells was removed and centrifuged at 1500 rpm for 5 minutes at 4°C. • The final digest was centrifuged at 1500 rpm for 10 min.
- 41. • The cell pellet was washed three times in PBS or serum free medium. • Cell suspensions were passed through a nitex nylon filter (mesh width 70 mm) and re-suspended in serum containing medium. • The cell viability was determined by trypan blue dye exclusion test in hemocytometric chamber.
- 42. Chondrocytes Monolayer Culture: • The cells isolated cartilage were seeded in 4 well culture plates at low density (4000 cell/cm²) in culture medium in an equal volume mix of ham’s F12 medium and Dulbecco's modified eagle medium (F12:DMEM). • Each culture mediums also contained Ascorbic acid (50µl/ml), penicillin (100µl/ml), streptomycin (100µl/ml), L-glutamine (200mM) and incubated in a CO₂ incubator at 5% CO₂, 37° C and saturated humidity for periods of up to 40 days. • The culture medium was changed twice or three times per week.
- 43. Morphology and Passage Chondrocytes: • The cell morphologic feature was examined daily by phase microscopy in an inverted microscope. • The cultures were regularly photographed for monitoring cell morphology. • When chondrocytes reached 70 to 90% confluency, the cells were detached mechanically, using trypsinization 1 to 2 min and harvested chondrocytes were washed and re-suspended in PBS than total cell number and their viability was assessed using the trypan blue test.
- 44. Human chondrocytes primary culture (passage zero) after 40 days showed different morphology feature in DMEM/F12 supplemented with different factors A: primary culture after 13 days B: primary culture after 25 days C: culture of 40 days D: chondrocytes culture
- 45. SANDWICH TECHNIQUE • ACI has traditionally been applied to treat relatively shallow lesions of articular cartilage without involvement of the subchondral bone. • For osteochondral defects of more than 8 to 10 mm in depth, bone grafting is recommended. • The bone graft may be performed at the time of biopsy and the implantation may be delayed to allow for bone graft consolidation.
- 46. • Alternatively, the “sandwich technique” has been utilized to replace bone and resurface the defect in a single step. • With this technique, the bone defect is filled with bone graft, periosteum is sutured on top of the bone graft at the level of the subchondral bone plate, a second layer of periosteum is placed over the cartilage defect, and the chondrocytes are then placed between the layers of periosteum.
- 48. Stages of ACI healing • Healing process has several stages. They include the • proliferative stage (0 to 6 weeks), • the transition stage (7 to 12 weeks), and • a remodelling and maturation stage which occurs over a prolonged period (13 weeks to 3 years)
- 49. Proliferative stage • During this stage, a primitive cell response occurs with tissue fill of the defect and poor integration to underlying bone or adjacent cartilage. • Mostly type I and some type II collagen is produced. • The tissue is soft and jelly-like and easily damaged
- 50. Transition phase • This marks the production of type II collagen framework and the early production of proteoglycans. • The proteoglycans, which form the matrix, help imbibe water to give cartilage its viscoelastic properties. • The tissue is not yet firm or well integrated and has the consistency of a firm gelatin. • It is milkable when probed with an arthroscopic nerve hook, indicating incomplete integration to underlying bone.
- 51. Stage of remodelling and maturation • The matrix proteins cross-link and stabilize in large aggregates. • The collagen framework reorganizes so as to integrate into the subchondral bone and form arcades of Benninghoff. • Usually by 4 to 6 months, the tissue has firmed up to a putty-like consistency and is integrated to the underlying bone. • At this stage, patients experience good symptom relief. • During this stage excessive activity may cause repair tissue degeneration or continued improvement in remodelling.
- 52. ONE YEAR ASSESSMENT • Radiographs – Alignment – Bone quality • MRI – Healing cartilage – Graft failure • Arthroscopy – Graft integrity – Pressure – Biopsy
- 54. FOLLOW UP: MRI
- 55. FOLLOW UP: ARTHROSCOPIC • Final appearance of the periosteum sutured over femoral condyle defect. The cartilage cells have been injected under the flap and the final suture placed to close the "cover" and provide a watertight seal.
- 56. • Arthroscopic appearance of the same area 12 months after Carticel™ implantation. The defect is no longer visible and there is now hyaline cartilage filling the original defect site.
- 57. REHABILITATION GUIDELINES • Immobilization: First 12-24 hours • (CPM): After 12-24 hours, for about 4 weeks • Complete joint loading: from about 5th week patella from about 8th week condyle • Back to sports: – Low impact → within 6 months – Repeated impact → from 8th month – High impact → from 10-12th month
- 58. ACI REHABILITATION Weight bearing • It is recommended to keep you in non-weight bearing until the second week after surgery (ACI). You can increase the weight bearing gradually and you may be able to sustain your full weight bearing after 6 to 12 weeks from surgery.
- 59. Range of motion • Recovery on your ROM (Range of Motion) is gradually increased with a continuous passive motion (CPM) machine and may be completed to 140 degrees of ROM at 6 weeks to 12 weeks after surgery
- 60. Indoor exercise • You can strenghthen your muscles surrounding the knee joint with a four point exercise, as well as isometric, hamstring and squatting exercises, from 4 weeks to 6 weeks after surgery. • You may start performing stationary bike activity without resistance and increase the resistance gradually.
- 61. Outdoor exercise • At 13 weeks after surgery you can start walking lightly and at 10 months after surgery you can perform jogging and then you may enjoy intensity exercise like playing tennis or volleyball from 18 months after surgery.
- 62. Rehabilitation Goals at 12 weeks after ACI • Full ROM (Range of Motion) • Minimal edema level • Minimal occasional pain • Pain free tolerance to transitional phase exercise with adequate stability and motor control
- 63. ADVANTAGES • Can produce hyaline-like cartilage. • Can fill defects regardless of size with functional repair tissue. • Moderate to large defects that have failed previous intervention. • Repair tissue which matures, rather than damage over time. • Expected outcome • Return to previous level of functioning
- 64. DISADVANTAGES • More invasive • Expense • Longer recovery
- 65. COMPLICATIONS • The overall failure rate is 10%. The two most common complications include : • loosening of the transplant tissue, • formation of fibrous tissue at the repair site and adhesions with return of pain. Other adverse events include : • post-op haematoma (big blood clot) • hypertrophic synovitis (angry knee) and superficial wound infection.
- 66. COMPARISON WITH OTHER METHODS OF TREATMENTS : Autologous Chondrocyte Implantation • Aims to increase the best condition for cartilage defect. Advantages: • Hyaline cartilage is formed • Permanent reconstructed cartilage tissue • Most valuable treatment
- 67. Abrasion arthroplasty • Aims to decrease the inflammation of the joint. Disadvantages: • Removes many cartilage fragments from the joint • Symptoms reoccur within one year
- 68. Drilling and Microfracture • Aims to generate a healing response. Disadvantages: • The healing response in inadequate • No hyaline cartilage is formed, but rather fibrocartilage • Has a limited lifespan of approximately one year • Rapid damage after such procedures can be expected
- 69. Perichondral Resurfacing Disadvantages: • Isolated cartilage defects are often too large to be covered by perichondrum • Long term follow-up of such procedures indicate that the implants undergo endochondral ossification
- 70. Synthetic Materials (i.e. Carbon Fiber Mesh) Disadvantages: • It often results in fibrous tissue formation • Not adequate biomechanically • Often the cause for synovitis in the joints
- 71. Osteocartiloginous Grafts • Aims to reconstruct joints. Disadvantages: • Unless fresh cartilage is transplanted, the cartilage is dead • Fresh grafts are not commonly used, as they inevitably carry a risk of disease transmission • Cyropreserved grafts can survive for many years, but ultimately damage