Brain Abscess Diagnosis and Treatment
•Download as DOCX, PDF•
2 likes•465 views

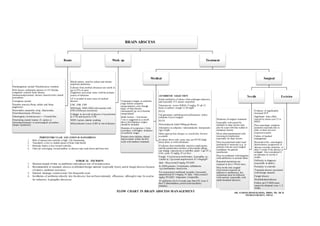
Brain abscesses can develop through hematogenous or contiguous spread from infections elsewhere in the body. Common causes include sinusitis, dental infections, and congenital heart defects. Diagnosis involves blood tests, MRI, and sometimes brain biopsy. Treatment consists of 6-8 weeks of IV antibiotics, along with needle aspiration or excision of the abscess depending on its size and location. The choice of antibiotics depends on suspected causative organisms but commonly includes vancomycin, metronidazole, and third generation cephalosporins. Surgical drainage or excision may be needed for large or multi-loculated abscesses.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Brain Abscess Diagnosis and Treatment
Similar to Brain Abscess Diagnosis and Treatment (20)
More from suresh Bishokarma
More from suresh Bishokarma (20)
Recently uploaded
Recently uploaded (20)
Brain Abscess Diagnosis and Treatment
- 1. BRAIN ABSCESS Route Hematogenous spread: Pneumococcus common Risk factors: pulmonary abscess or AV fistulas, congenital cyanotic heart disease, immunocompromised, chronic sinusitis/otitis, dental procedures. Contiguous spread: Purulent sinusitis (Strep. milleri and Strep. anginosus) Mastoiditis:(anaerobic strep., Bacteroides, Enterobacteriaceae (Proteus) Odontogenic (Actinomyces)—> Frontal lobe. Penetrating cranial trauma: (S. aureus or Enterobacteriaceae) or neurosurgical procedure (Staph. Epidermis) Work up Blood culture: send for culture and initiate empirical antibiotics Cultures from cerebral abscesses are sterile in up to 25% of cases Organisms recovered varies with the primary source of infection: LP is avoided in most cases of cerebral abscess. CBC, ESR, CRP MRI brain: MRS, MRI with contrast with DWI (Diffusion restriction) Collagen in thewall of abscess is hypointense in T1W and hyper in T2W. MRS: Lactate, alanine peaking. MR perfusion:Lower rCBV in rim of abscess Treatment Medical Treatment is begun in cerebritis stage (before complete encapsulation), even though many of theselesions subsequently go on to become encapsulated. Small lesions: <3cm lesion 3 cm is suggested as a cutoff, above this diameter surgery should be included. Duration of symptoms ≤ 2wks (correlates with higher incidence of cerebritis stage). Patients show definite clinical improvement within thefirst week with medical treatment ANTIBIOTIC SELECTION Initial antibiotics of choice when pathogen unknown, and especially if S. aureus suspected: Vancomycin: covers MRSA:15 mg/kg IV q8-12 hours to achieve trough 15-20 mg/dl PLUS 3rd generation cephalosporin (ceftriaxone); utilize cefepime if post-surgical PLUS Metronidazole.Adult:500mg q6-8hours Alternative to cefepime +metronidazole: meropenem 2gm IVq8h Make appropriate changes as sensitivities become available If culture shows only strep, may use PCNG (high dose) alone or with ceftriaxone If cultures show methicillin sensitive staph aureus and the patient does not have a beta lactam allergy, can change vancomycin to nafcillin (adult: 2 gm IV q 4 hrs. peds:25 mg/kg IV q 6 hrs) Fungal: Cryptococcus neoformans, Aspergillus sp., Candid as: Liposomal amphotericin B 3-4mg/kgIV daily +flucytosine25 mg/kg PO QID. In AIDS patients:Toxoplasma: sulfadiazine +pyrimethamine+leucovorin. For suspected or confirmed nocardia: Liposomal amphotericin B 3-4mg/kg IV daily +flucytosine25 mg/kg PO QID + Imipenem Ampicillin. IV antibiotics for 6–8 weeks may then D/C even if the CT abnormalities persist (neovascularity remains). Surgical Needle Mainstay of surgical treatment. Especially well-suited for multiple or deep lesions may also be used with thin walled or immature lesions Most often implemented with stereotactic localization especially for deep lesions May beperformed under local anesthesia if necessary (e.g. in patients who are poor surgical candidates for general anesthesia). May becombined with irrigation with antibiotics or normal saline. Repeated aspirations are required in up to 70%of cases. May bethe only surgical intervention required (in addition to antibiotics), but sometimes must be followed with excision (especially with multi-loculated abscess). Excision Evidence of significantly increased ICP. Significant mass effect exerted by lesion (on CT or MRI) Poor neurologic condition (patients responds only to pain, or does not even responseto pain) Failure of medical management: Resistant to Rx: neurological deterioration, progression of abscess towards ventricles, or after 2 weeks if the abscess is enlarged. Also considered if no decrease in sizeby 4 weeks. Difficulty in diagnosis (especially in adults). Proximity to ventricle Traumatic abscess associated with foreign material Fungal abscess Multilobulated abscess Follow-up CT/MRI scans cannot be obtained every 1–2 weeks. SURGICAL EXCISION: 1. Shortens length of time on antibiotics and reduces risk of recrudescence. 2. Recommended in traumatic abscess to debrided foreign material (especially bone), and in fungal abscess because of relative antibiotic resistance 3. External drainage: controversial. Not frequently used. 4. Instillation of antibiotics directly into the abscess:has not been extremely efficacious, although it may be used as for refractory Aspergillus abscesses FLOW CHART IN BRAIN ABSCESS MANAGEMENT PERIVENTRICULAR LOCATION IS DANGEROUS 1. Risk of ruptureinto ventricle is high: Life threatening 2. Vascularity is less in medial aspect of brain than lateral 3. Reticular matrix is less toward ventricle, 4. Fiber are converging toward midline so abscess may track down and brust into ventricl DR. SURESH BISHOKARMA, MBBS, MS, MCH NEUROSURGEON, NEPAL