This document provides an overview of appendicitis including:
1. The introduction summarizes appendicitis as the most common urgent surgery and discusses its propensity to form tumors.
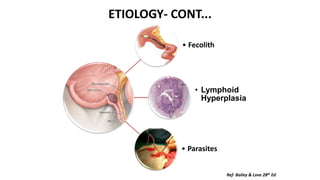
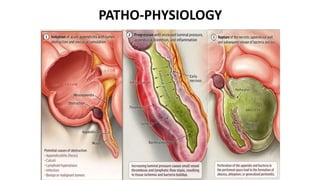
2. The pathophysiology section discusses the etiology of appendicitis including fecoliths, lymphoid hyperplasia, and parasites.
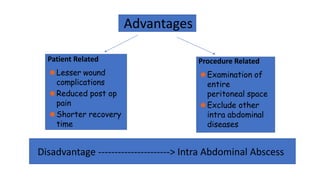
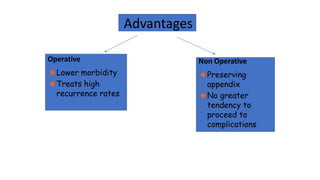
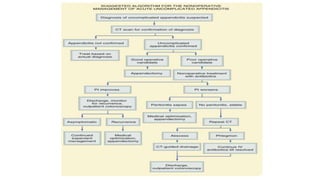
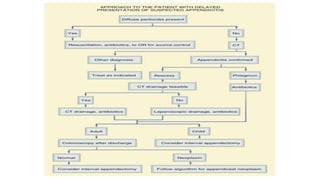
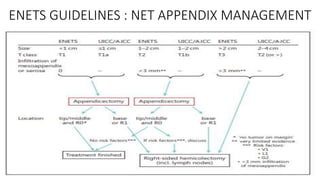
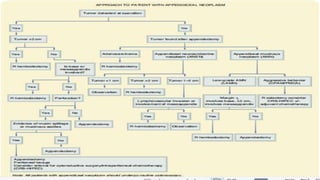
3. Management is discussed including laparoscopic versus open appendectomy, non-operative versus operative treatment, and considerations for delayed presentation and normal appearing appendices.


![A COMPLEX DISEASE ENTITY
Teng TZJ, Thong XR, Lau KY, Balasubramaniam S, Shelat VG. Acute appendicitis–advances and controversies. World J
Gastrointest Surg 2021; 13(11): 1293-1314 [PMID: 34950421 DOI: 10.4240/wjgs.v13.i11.1293]](https://image.slidesharecdn.com/appendixdraft-230309151956-fb361def/85/APPENDIX-DRAFT-pptx-41-320.jpg)






































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

















