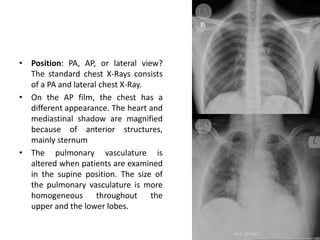
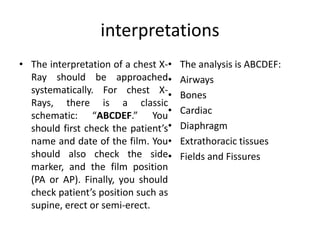
There are three types of chest films: anteroposterior (AP), posteroanterior (PA), and lateral. The ideal timing is at the end of inspiration when the patient holds their breath and the x-ray tube is 180cm away. Image quality is assessed using the "RIPE" mnemonic of rotation, inspiration, position, and exposure to ensure visibility of key structures like the heart and vertebrae. Interpretation follows the "ABCDEF" schema of checking the airways, bones, cardiac, diaphragm, extrathoracic tissues, and fields and fissures for any abnormalities.