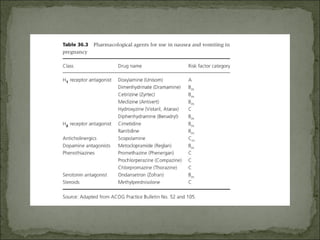
The document discusses the relationship between vomiting and nausea during pregnancy, detailing physiological and pathological aspects such as hyperemesis gravidarum, which affects 1 in 200 pregnant women. It outlines causes, diagnostic investigations, and treatment options, emphasizing the role of vitamin B6 and ginger in managing symptoms. Additionally, the text highlights the importance of recognizing different types of vomiting to identify underlying conditions.













































![[Aafp2014] nausea and vomiting of pregnancy](https://cdn.slidesharecdn.com/ss_thumbnails/aafp2014nauseaandvomitingofpregnancy-170605031124-thumbnail.jpg?width=640&height=640&fit=bounds)































