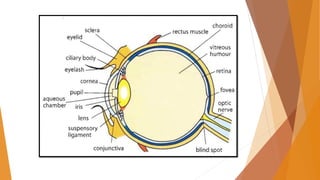
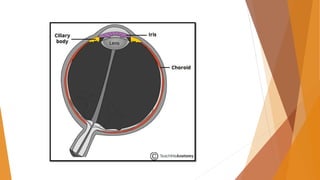
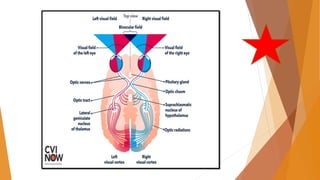
The document summarizes the structure and function of the human eye. It describes the three layers that make up the eyeball - fibrous, vascular and nervous layers. The fibrous layer includes the sclera and cornea. The vascular layer includes the choroid, ciliary body and iris. The nervous layer is the retina. It also explains key parts of the eye like the iris, lens, vitreous humor and aqueous humor. The retina contains photoreceptors that convert light to neural signals sent to the brain via the optic nerve. The visual pathway and common refractive errors are also summarized.