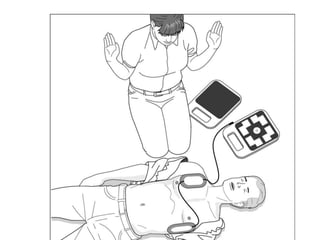
This document provides guidance on first aid procedures for a variety of common medical emergencies. It details how to measure vital signs, assess an unconscious person, perform CPR, use an AED, and treat choking, burns, wounds, fractures, allergic reactions, and more. Proper first aid actions can help stabilize a person and save their life until emergency medical help arrives.