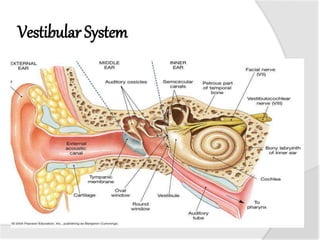
The vestibular system helps control balance and eye movements. Damage to the system can cause vestibular disorders with symptoms like vertigo, dizziness, imbalance, and vision or hearing changes. Common vestibular disorders include BPPV, labyrinthitis, and Meniere's disease. Assessment of vestibular function includes tests of vision, balance, neurological function, and vestibular reflexes to evaluate disorders like BPPV, labyrinthitis, and other conditions that affect the inner ear and balance.