This document discusses various types of vascular tumors, including benign tumors like hemangiomas and lymphangiomas, intermediate tumors like hemangioendotheliomas, and malignant tumors such as Kaposi sarcoma and angiosarcomas. It covers the histological and clinical features used to classify and diagnose these different vascular neoplasms. Key information includes that benign tumors form well-organized vessels, while malignant tumors are more cellular and proliferative without such organization. Immunohistochemistry can help identify the endothelial cell origin of these proliferations.



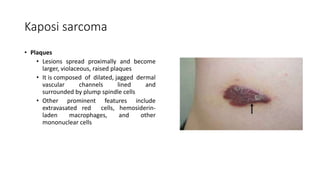







![Neoplasia [part 1]](https://cdn.slidesharecdn.com/ss_thumbnails/neoplasiapart1-190918152450-thumbnail.jpg?width=640&height=640&fit=bounds)




























































