Normal Vascular structure
Vasculature is divided into arterial and
venous components joined by a network
of capillaries.
3.
Introduction
VASCULOGENESIS
De novodevelopment of
blood vessels from
primitive endothelial
cells.
Early embryogenesis.
ANGIOGENESIS
Formation of new
microvessels from
differentiated
endothelium.
During embryogenesis
and postnatal state.
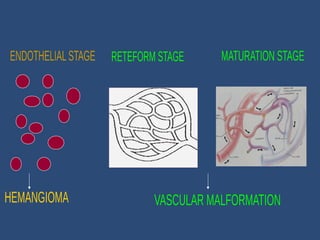
Hemangioma Vascular
malformation
Appearsweeks after
birth
Rapid growth
Spontaneous involution
Abnormality of
endothelial cell
proliferation
Results from increased
number of capillaries
Often circumscribed
Usually present at birth
Progressive
enlargement
No involution
Abnormality of vessel
morphogenesis
Results from dilatation
of arterioles,
veins/capillaries
Poorly circumscribed
7.
Hemangioma
Most commonsoft tissue tumor during infancy and
childhood.
Most hemangiomas are superficial lesions that have a
predilection for the head and neck region, but they may
also occur internally, such as in the liver.
Composed of capillary vessels arranged in lobules, which
are subserved by a feeder vessel.
Most cases persist if untreated but have limited growth
potential but some vascular tumors (infantile
hemangioma) regress altogether.
Usually 80%of all hemangiomas are single lesions,
but 20% of affected infants develop multiple
tumors
In oral cavity, it can involve lip(63%), buccal
mucosa(14%), lateral border of tongue(14%),
maxillary sinus, maxilla, mandible and parotid
glands.
Demographics
Site
Oral hemangiomasrepresent 14% of all
human hemangiomas
60% hemangiomas are located in head and
neck area
25% occur on the trunk
15% on the extremities
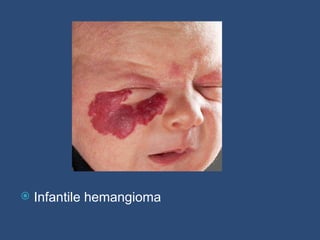
ORAL MANIFESTATIONS:
Appear as a flat or raised lesion of the
mucosa, usually deep red or bluish red and
seldom well circumscribed.
They are readily compressible and fills
slowly when released.
Site:
Lips, Tongue, Buccal mucosa, Palate
The tumor presents at birth or shortly thereafter
as a red-purple macule that slowly becomes raised
and then tends to regress in over 70% of cases
after a period of months to years.
15.
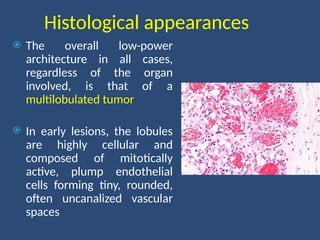
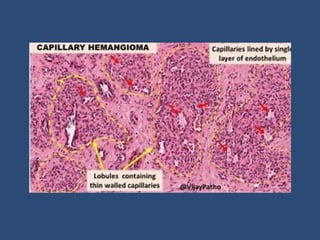
Histological appearances
Theoverall low-power
architecture in all cases,
regardless of the organ
involved, is that of a
multilobulated tumor
In early lesions, the lobules
are highly cellular and
composed of mitotically
active, plump endothelial
cells forming tiny, rounded,
often uncanalized vascular
spaces
17.
As lesionsmature, the vessels become
canalized and more easily recognized, then
often showing congested lumina and flat
endothelial cells.
Older lesions become progressively fibrotic
with almost complete regression or absence
of the vascular elements.
19.
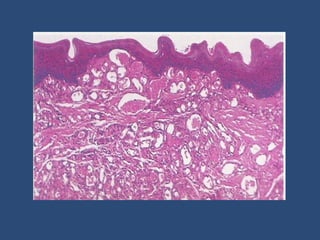
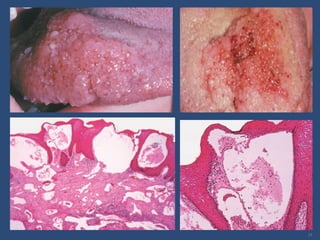
LOBULAR CAPILLARY HEMANGIOMA/PYOGENIC
GRANULOMA
The classical appearance is that of a solitary, rapidly
growing, ulcerated, bleeding, polypoid blue-red
nodule which is usually less than 2cm in diameter
H/F-
Ulcerated epithelium, prominent acute inflammatory
infiltrate
Core of tumor shows lobules of small capillaries, with
or without discernible lumina, lined by prominent
endothelial cells
Stroma is loose and edematous
Old lesions can show marked fibrosis.
22.
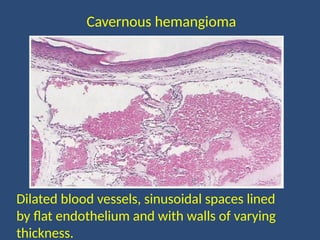
Cavernous hemangioma
Clinicalfeatures are similar to capillary hemangioma,
however, these lesions tend to be larger, deeper and
less well circumscribed
Histologic appearances
Consist of poorly circumscribed, irregularly dilated
blood vessels lined by flat endothelium and with walls
of varying thickness.
Areas resembling capillary hemangioma often can be
found focally, especially in the superficial portion
23.
Dilated blood vessels,sinusoidal spaces lined
by flat endothelium and with walls of varying
thickness.
Cavernous hemangioma
Lymphangioma
Lymphangiomas areuncommon, benign
malformations of the lymphatic system
True neoplasm/hamartoma?
Lymphangiomatosis- multiple lesions seen in infancy
and childhood. It is a potentially life-threatening
disease with visceral involvement
Classification-
Simple
Cavernous
Cellular or hypertrophic
Diffuse systemic
Cystic hygroma
27.
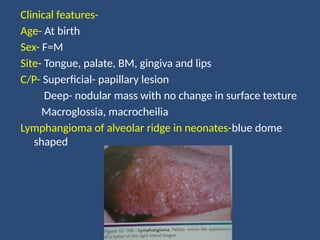
Clinical features-
Age- Atbirth
Sex- F=M
Site- Tongue, palate, BM, gingiva and lips
C/P- Superficial- papillary lesion
Deep- nodular mass with no change in surface texture
Macroglossia, macrocheilia
Lymphangioma of alveolar ridge in neonates-blue dome
shaped
28.
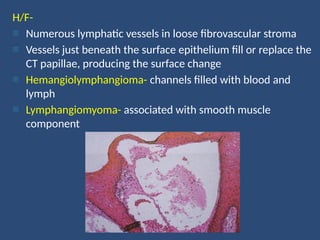
H/F-
- Numerous lymphaticvessels in loose fibrovascular stroma
- Vessels just beneath the surface epithelium fill or replace the
CT papillae, producing the surface change
- Hemangiolymphangioma- channels filled with blood and
lymph
- Lymphangiomyoma- associated with smooth muscle
component
Hemangiopericytoma
Benign tumorof pericytes
Distinct entity?
Clinical features-
Age- 2nd
-7th
decade
Sex- F=M
C/P- Rapidly enlarging red/bluish mass
- Soft and rubbery in consistency
- Infantile type- rapid rate of enlargement
32.
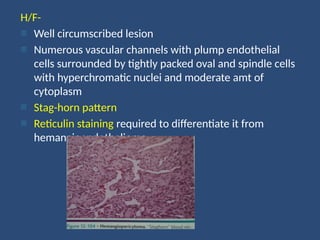
H/F-
- Well circumscribedlesion
- Numerous vascular channels with plump endothelial
cells surrounded by tightly packed oval and spindle cells
with hyperchromatic nuclei and moderate amt of
cytoplasm
- Stag-horn pattern
- Reticulin staining required to differentiate it from
hemangioendothelioma
Hemangioendothelioma
Vascular lesionswith a biologic behavior
intermediate between hemangioma &
angiosarcoma
Clinical features-
Age- Infants
Sex- Female>Male
Site- skin and soft tissues, especially in the head and
neck area.
Commonest location in the oral cavity- lip, palate,
gingiva, tongue
C/P- similar to hemangioma
35.
H/P-
Poorly circumscribedlesion characterized by the
proliferation of endothelial cells and multiple
vascular spaces
Variants-
Epitheloid
Kaposiform
Polymorphous
Spindle cell








































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













