The document provides a comprehensive overview of aortic regurgitation (AR), detailing its anatomy, epidemiology, etiology, pathophysiology, clinical features, diagnostic techniques, management strategies, and treatment options. It discusses both chronic and acute AR, highlighting the clinical implications of symptoms, echocardiographic findings, and the significance of monitoring and intervention. The document emphasizes the necessity for timely surgical intervention in acute cases, along with the gradual monitoring and management of chronic cases based on severity and patient symptoms.




































![Treatment of Chronic Aortic Regurgitation
Medical Therapy
• No specific therapy to prevent disease progression in chronic AR
• RCT of DHP-CCB and (ACE inhibitors have not shown consistent clinical
benefit in terms of blunting progression of LV dilation or delaying in need for
AVR.
• Treat hypertension (systolic blood pressure [SBP] >140 mm Hg), coronary
artery disease (CAD), atrial arrhythmias, and any other cardiovascular
comorbidities
• Chronic medical therapy may be necessary for some patients
• who refuse surgery
• have a prohibitive risk of surgery because of comorbid conditions](https://image.slidesharecdn.com/aorticregurg-240714152623-7813bf55/75/valvular-heart-diseaseAORTIC-REGURGITATION-pptx-43-2048.jpg)

![Recommendations for physical activity and exercise:
• Athletes with greater-than-mild AR should be evaluated yearly
• Exercise testing to at least the level of activity achieved in competition and training is helpful
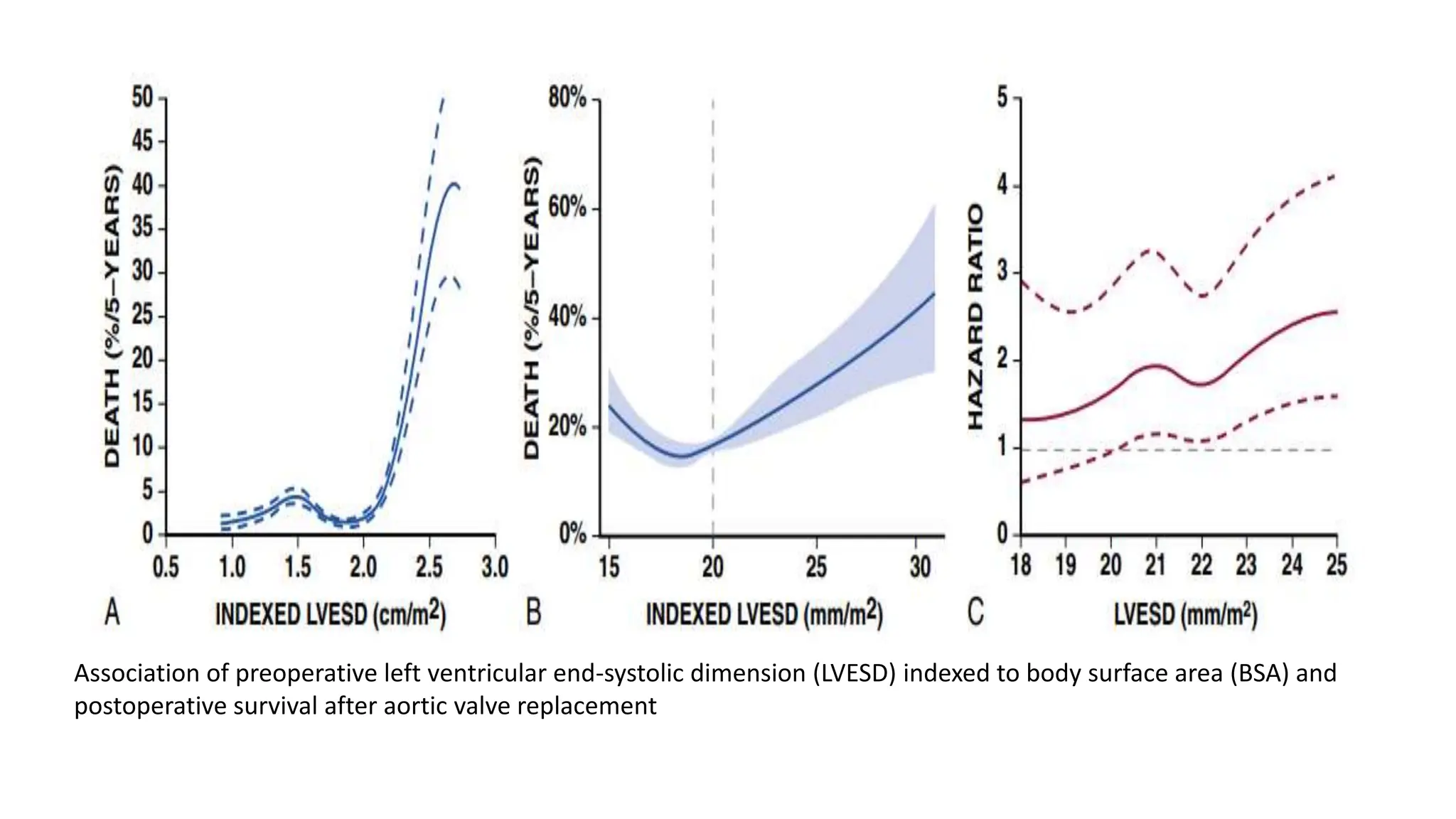
• Stage B with normal LVEF and normal or mildly increased LV end-systolic dimension (LVESD)
with normal exercise tolerance on exercise testing can participate in all competitive sports.
• Athletes with mild to moderate degrees of AR with normal LVEF and moderately increased
LVESD (<50 mm [men], <40 mm [women], or <25 mm/m2 [either sex]) with normal exercise
tolerance on exercise testing can participate in all competitive sports.
• Athletes with severe AR, LVEF ≥50 percent, and LVESD <50 mm (men), <40 mm (women), or
<25 mm/m2 (either sex) with normal exercise and no progression of AR severity or degree of
increase in LVESD on serial Doppler echocardiography may continue to participate in all
competitive sports.
• It is reasonable for athletes with AR and aortic dimensions of 41 to 44 mm to participate in
sports with low risk of bodily contact.
• Athletes with severe AR and symptoms (stage D), or LV systolic dysfunction with ejection
fraction <50 percent (stage C2), or LVESD >50 mm or >25 mm/m2 (stage C2), or severe increase
in LV end-diastolic dimension (LVEDD >70 mm or ‡35.3 mm/m2 [men], >65 mm or ‡40.8
mm/m2 [women]) should not participate in competitive sports.](https://image.slidesharecdn.com/aorticregurg-240714152623-7813bf55/75/valvular-heart-diseaseAORTIC-REGURGITATION-pptx-45-2048.jpg)