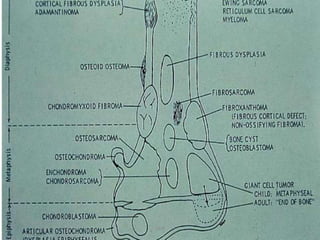
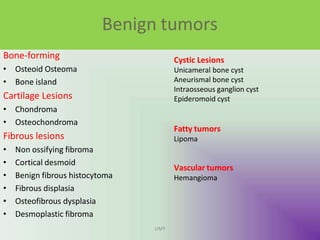
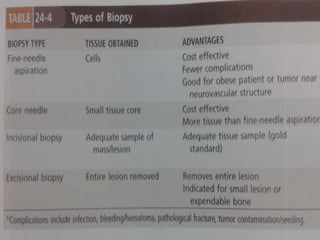
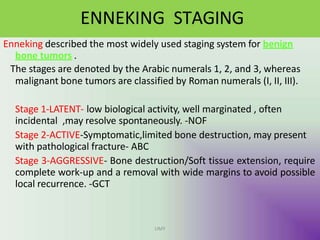
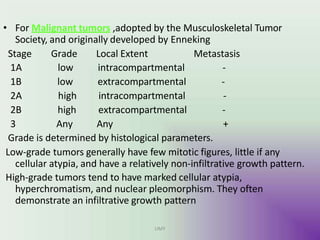
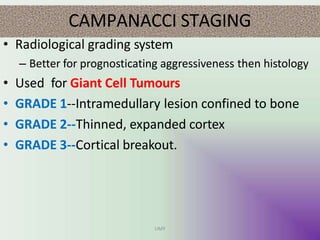
Benign bone tumors are diverse in morphology and biological potential. Most bone tumors are benign lesions seen in patients under 30 years old. Radiology is important for determining the exact location, extent of growth, and aggressiveness of bone tumors. The best test for diagnosis is a biopsy, as it confirms if a tumor is malignant or benign and determines the bone cancer type and stage. There are several classification systems for bone tumors, including the Enneking and Campanacci staging systems, which help determine prognosis and appropriate treatment.