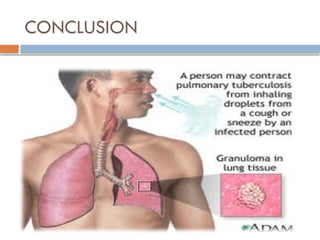
Pulmonary tuberculosis (TB)
DEF:Tuberculosis is the infectious disease primarily
affecting lung parenchyma is most often caused
by mycobacterium tuberculosis.it may spread to
any part of the body including
meninges,kidney,bones and lymph nodes.
It’s the one of the most prevalent infections of human beings
and contributes considerably to illness and death around the
world . It is spread by inhaling tiny droplets of saliva from
the coughs or sneezes of an infected person . It is slowly
spreading ,chronic , granulomatous bacterial infection
characterized by gradual weight loss
CLASSIFICATION
Class I(TB exposure)
(+) exposure
(-) Mantoux tuberculin test
(-) signs and symptoms suggestive of TB
(-) chest radiograph
5.
CLASSIFICATION
Class II(TB infection)
(±) exposure
(+) Mantoux tuberculin test
(-) signs and symptoms suggestive of TB
(-) chest radiograph
6.
CLASSIFICATION
Class III(TB disease)
Has three or more of the ff. criteria
(+) history of exposure to an adult/adolescent with active TB disease
(+) Mantoux tuberculin test
(+) signs and symptoms suggestive of TB
Cough/wheezing > 2 weeks; fever > 2 weeks
Painless cervical and/or other lymphadenopathy
Poor weight gain; failure to make a quick return to normal after an
infection (measles, tonsillitis, whooping cough) or failure to respond to
approriate antibiotic therapy (pneumonia, otitis media)
Abnormal Chest radiograph
Laboratory findings suggestive of TB (histological, cytological,
biochemical, immunological or molecular)
7.
CLASSIFICATION
Class IV(TB inactive)
A child/adolescent with or without history of previous
TB and any of the ff:
(±) previous chemotherapy
(+) radiographic evidence of healed/calcified TB
(+) Mantoux tuberculin test
(-) signs and symptoms suggestive of TB
(-) smear/culture for M. tuberculosis
Risk Factors
Age:infants and adolescents are at highest risk of
disease
Close contact with an untreated sputum positive
patient
Impaired host defenses: immunodeficiency states,
particularly that associated with HIV infection;
immunosuppression related to accompanying viral
infection, or drug induced; malnutrition.
10.
Risk Factors
Personswhose tuberculin skin test results converted to (+) In
the past 1-2 years.
Persons who have CXR suggestive of old TB.
IMMUNO COMPROMISED STATUS
(ELDERLY,CANCER).
DRUG ABUSE AND ALCOHOLISM.
PEOPLE LACKING ADEQUATE HEALTH CARE.
IMMIGRANTS FROM COUNTRIES WITH HIGHER
INCIDENCE OF TB.
INSTITUTIONALISATION(LONG TERM CARE
FACILITIES).
11.
PATHOPHYSIOLOGY
(INITIAL INFECTIONOR PRIMARY INFECTION)
ENTRY OF MICRO ORGANISM THROUGH DROPLET NUCLEI
BACTERIA IS TRANSMITTED TO ALVEOLI THROUGH AIRWAYS
DEPOSITION AND MULTIPLICATION OF BACTERIA
BACILLI ARE ALSO TRANSPORTED TO OTHER PARTS OF THE BODY
THROUGH BLOOD STREAM AND LYMPHNODE
INFLAMMATION
12.
PATHOPHYSIOLOGY
PHAGOCYTOSIS BYNEUTROPHILS AND MACROPHAGES
ACCUMULATION OF EXUDATE IN ALVEOLI
BRONCHO PNEMONIA
NEW TISSUE MASSES OF LIVE AND DEAD BACILLI ARE SURROUNDED BY
MACROPHAGES WHICH FORM A PROTECTIVE MASS AROUND GRANULOMAS
GRANULOMAS THEN TRANSFORMS TO FIBROUS TISSUE MASS AND CENTRAL
PORTION OF WHICH IS CALLED GHON TUBERCLE
13.
PATHOPHYSIOLOGY
THE MATERIAL(BACTERIA AND MACROPHAGES
BECOMES NECROTIC FORMING CHEESY MASS
MASS BECOMES CALCIFIED AND BECOMES
COLAGENOUS SCAR
BACTERIA BECOME DORMANT AND NO
FURTHER PROGRESSION OF ACTIVE DISEASE
(ACTIVE DISEASE OR RE INFECTION)
INADEQUATE IMMUNE RESPONSE
ACTIVATION OF DORMANT BACTERIA
14.
PATHOPHYSIOLOGY
GHON TUBERCLEULCERATES AND RELEASING CHEESY MATERIAL INTO
BRONCHI
BACTERIA THEN BECOME AIRBORNE RESULTING IN FURTHER SPREAD OF
INFECTION
ULCERATED TUBERCLE HEALS AND BECOMES SCAR TISSUE
INFECTED LUNG BECOME INFLAMMED
FURTHER DEVOLOPMENT OF PNEUMONIA AND TUBERCLE FORMATION
UNLESS THE PROCESS IS ARRESTED IT SPREADS DOWNWARDS TO THE HILUM
OF LUNGS AND LATER EXTENDS TO ADJASCENT LOBES
15.
CLINICAL MANIFESTATIONS
CONSTITUTIONAL SYMPTOMS
Anorexia
Low grade fever
Night sweats
Fatique
Weight loss
PULMONARY SYMPTOMS
Dyspnea
Non resolving bronchopneumonia
Chest tightness
Non productive cough
Mucopurulent sputum with hemoptpysis
Chest pain
EXTRA PULMONARY SYMPTOMS
Pain
Inflammation
16.
ASSESSMENT AND DIAGNOSTICFINDINGS
HISTORY COLLECTION
PHYSICAL EXAMINATION
Clubbing of the fingers or toes (in people with advanced disease)
Swollen or tender lymph nodes in the neck or other areas
Fluid around a lung (pleural effusion)
Unusual breath sounds (crackles)
IF MILIARY TB;
A physical exam may show:
Swollen liver
Swollen lymph nodes
17.
ASSESSMENT AND DIAGNOSTICFINDINGS
Tests may include:
Biopsy of the affected tissue (rare)
Bronchoscopy
Chest CT scan
Chest x-ray
Interferon-gamma release blood
test such as the QFT-Gold test
to test for TB infection
Sputum examination and cultures
Thoracentesis
Tuberculin skin test (also called a PPD test)
18.
COMPLICATIONS
Bones. Spinalpain and joint destruction may
result from TB that infects your bones(TB spine or
potss spine)
Brain(meningitis)
Liver or kidneys
Heart(cardiac tamponade)
Pleural effusion
Tb pneumonia
Serious reactions to drug therapy(hepato
toxicity;hypersentivity)
19.
MEDICAL MANAGEMENT
PULMONARYTB is treated primarily with antituberculosis
agents for 6 to 12 months.
Pharmacological management
FIRST LINE ANTITUBERCULAR MEDICATIONS
Streptomycin
Isoniazid or INH(Nydrazid)
Rifampin
Pyrazinamide
Ethambutol(Myambutol)
20.
MEDICAL MANAGEMENT
SECONDLINE MEDICATIONS .
Capreomycin
Ethionamide
Paraaminosalycilate sodium
Cycloserine
Vitamin b(pyridoxine) usually adminstered
with INH
21.
MEDICAL MANAGEMENT
THIRDLINE DRUGS
Other drugs that may be useful, but are not
on the WHO list of SLDs:
Rifabutin
Macrolides:e.g.,clarithromycin (CLR)
Linezolid(LZD)
Thioacetazone(T)
Thioridazine
Arginine
22.
MULTIDRUG THERAPY
Multiple-drugtherapy to treat TB means
taking several different antitubercular
drugs at the same time.
The standard treatment is to take isoniazid,
rifampin, ethambutol, and pyrazinamide for
2 months. Treatment is then continued for
at least 4months with fewer medicines








































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


