Downloaded 18 times





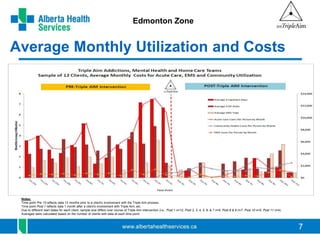

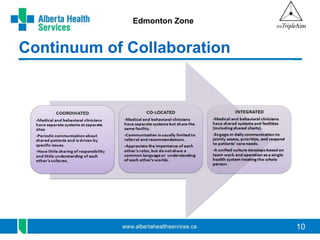


The document discusses the Triple Aim initiative in the Edmonton Zone. The Triple Aim is a collaborative with the Institute for Healthcare Improvement that aims to 1) improve population health, 2) improve care experiences, and 3) reduce costs. It focuses on understanding and meeting the needs of those in the top 5% of healthcare costs, including those experiencing homelessness or other social determinants of health issues. Challenges include transitions of care between providers and systems not sharing information well. The initiative uses case management and integrated services to improve outcomes while reducing costs over time for those engaged in the program. Learning includes the importance of permanent supportive housing and other community services for reducing acute care utilization and costs.



































































