Download as PDF, PPTX

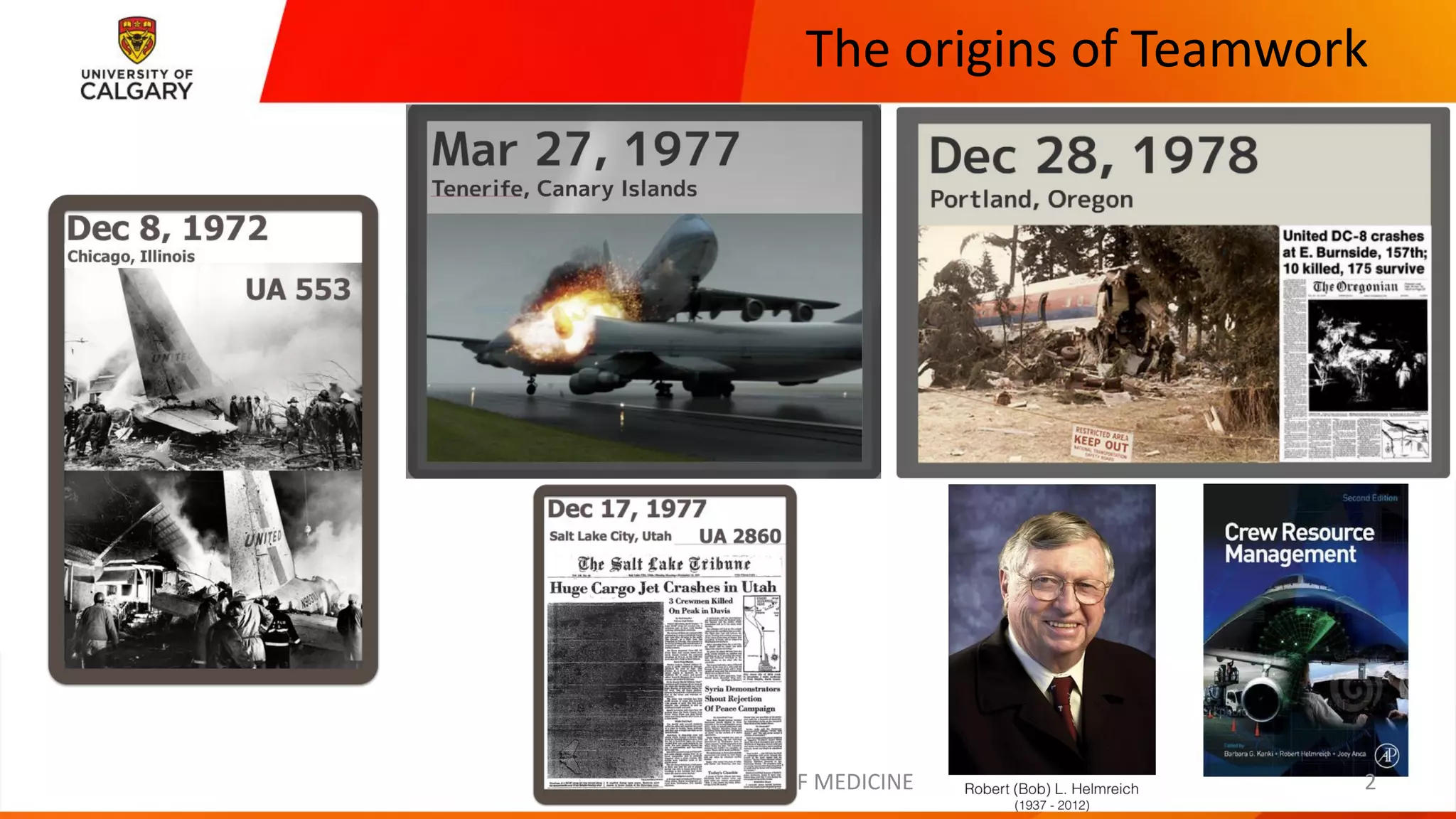
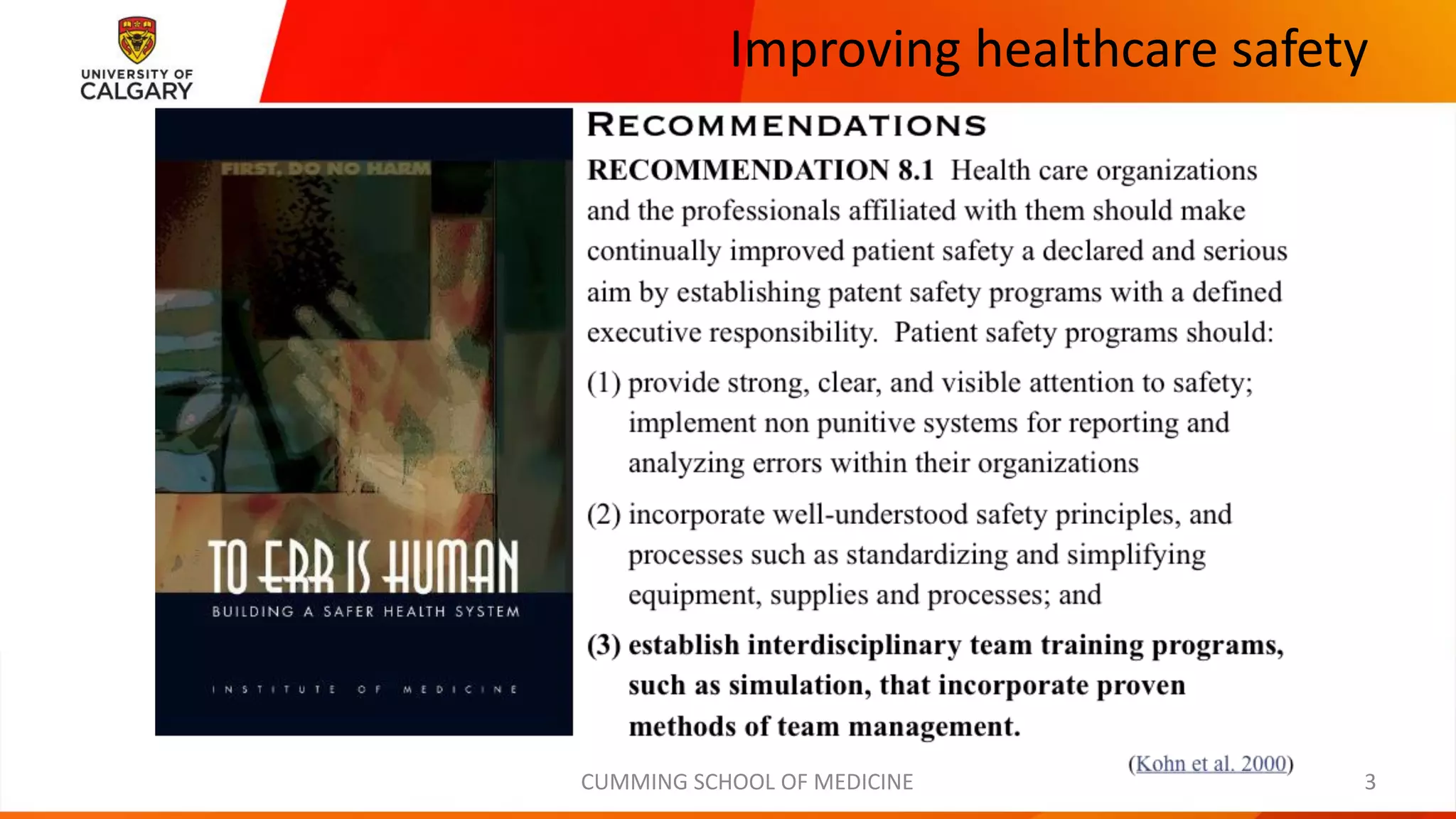
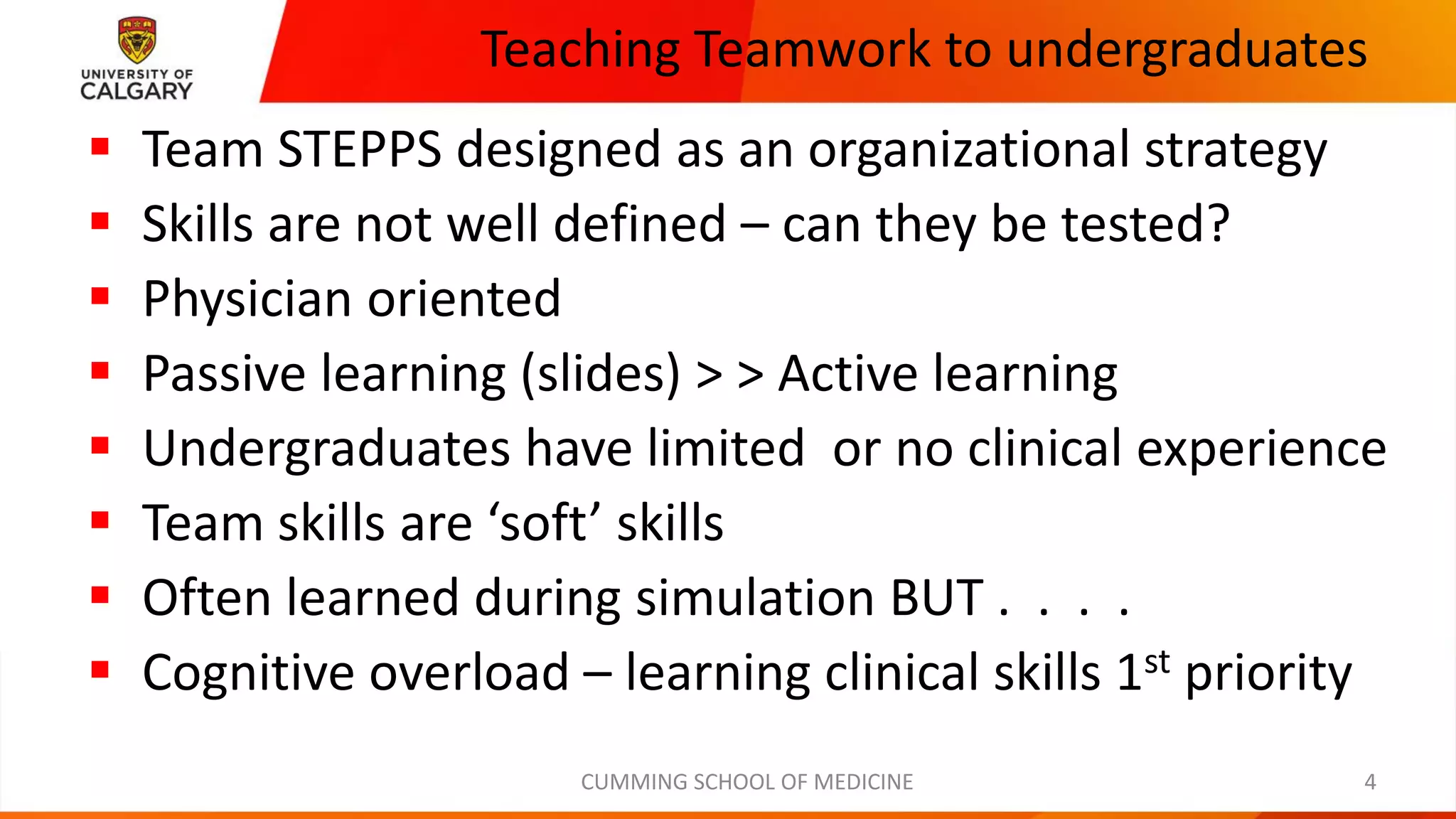
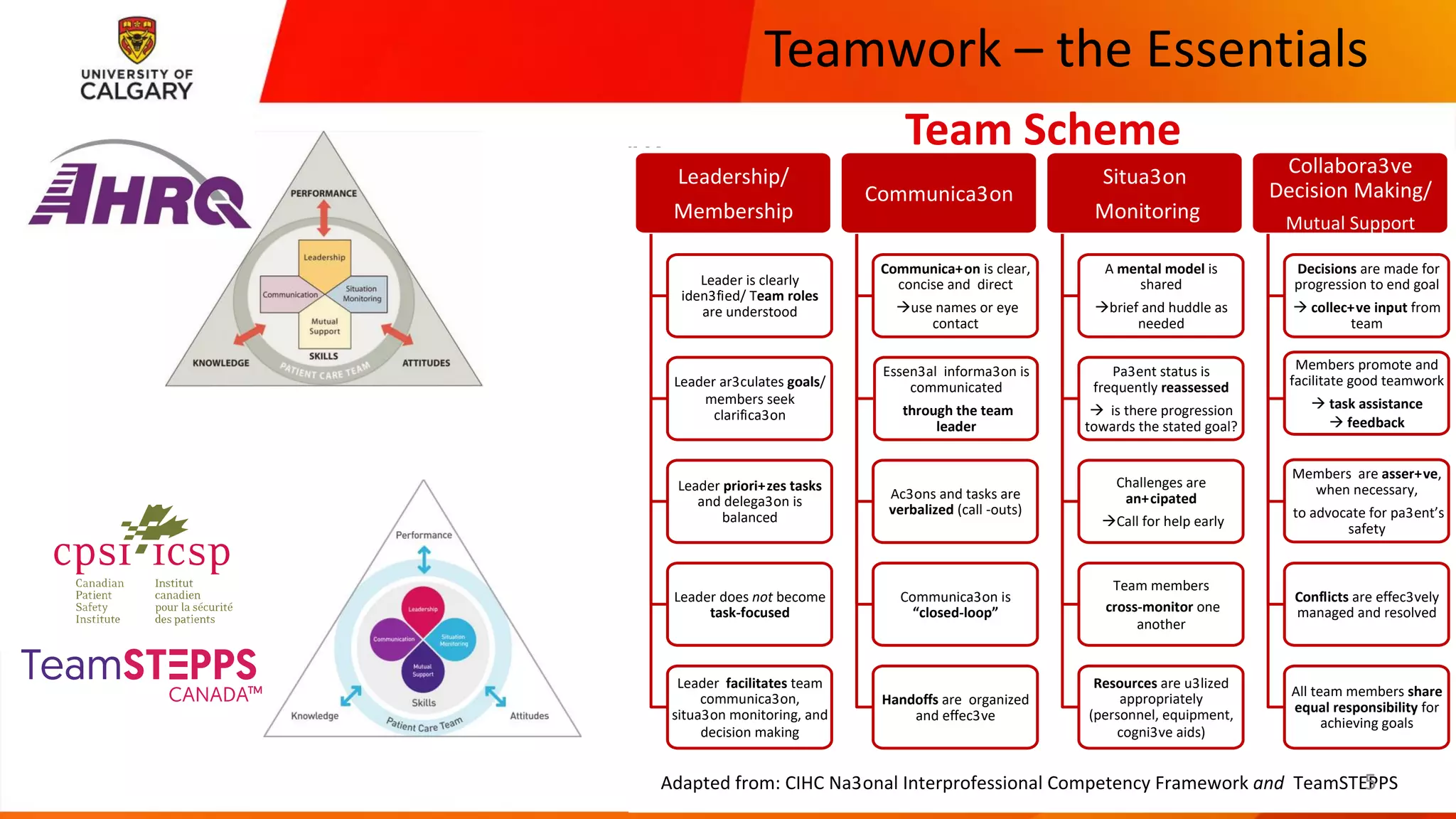
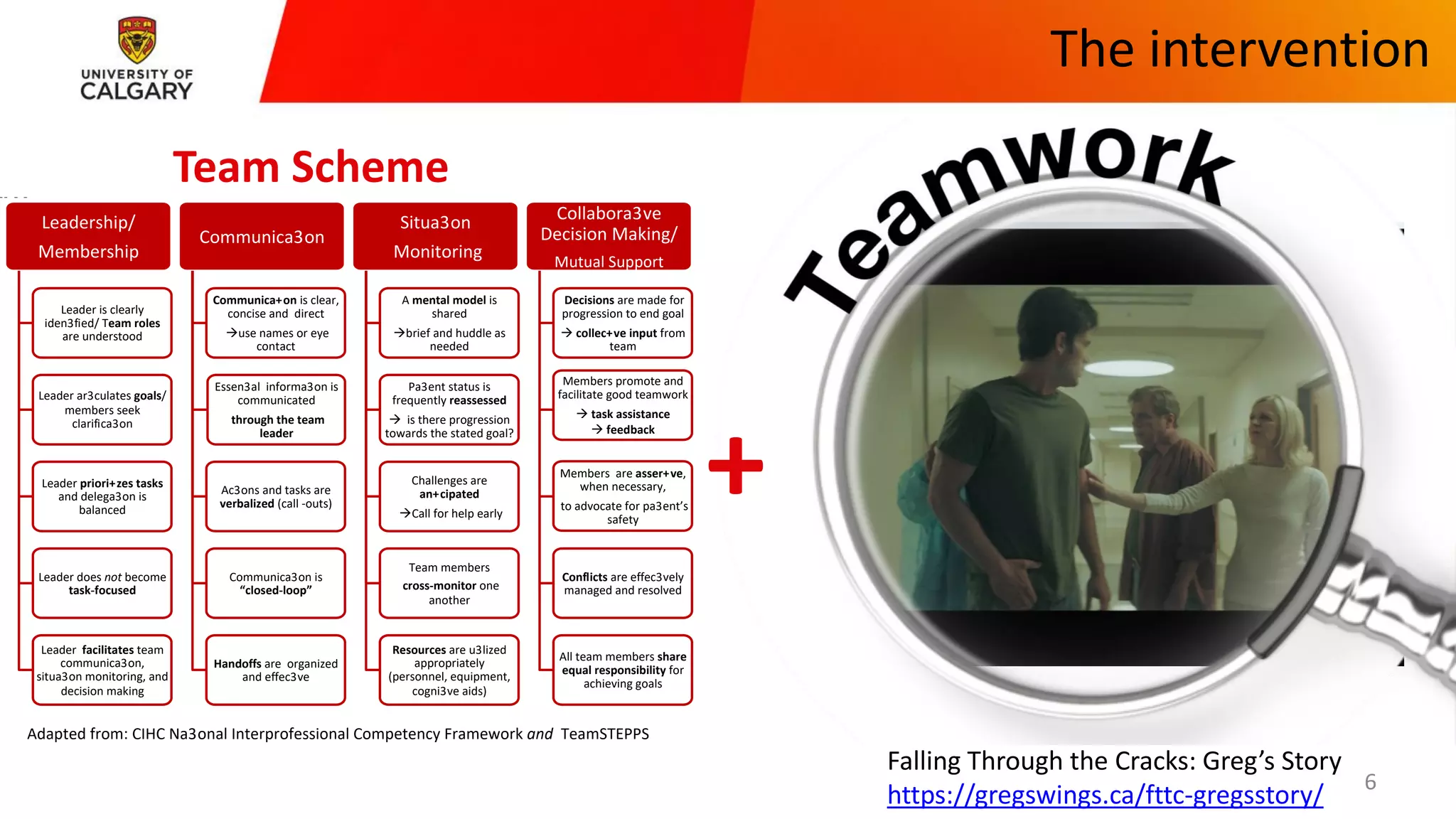
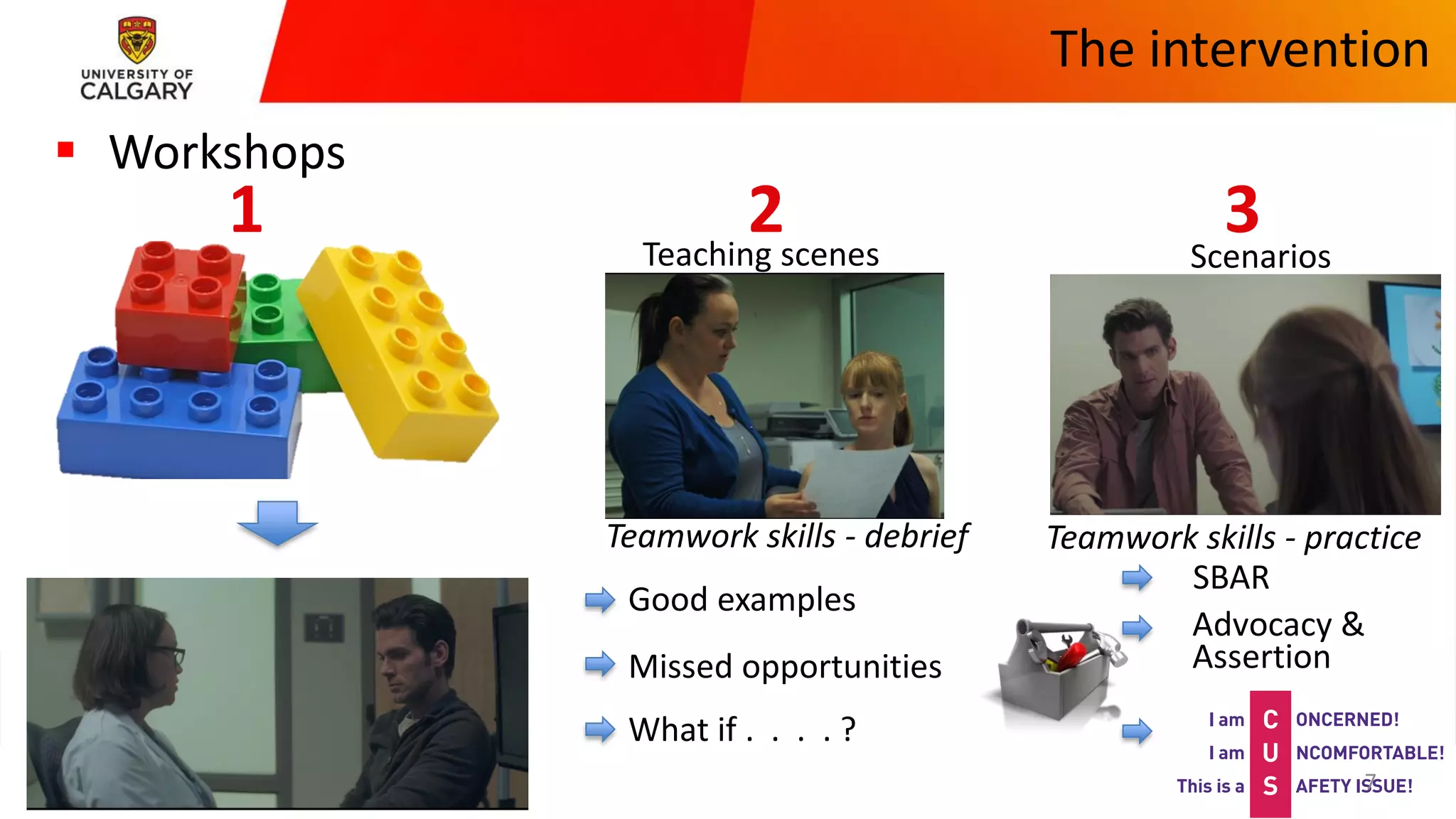
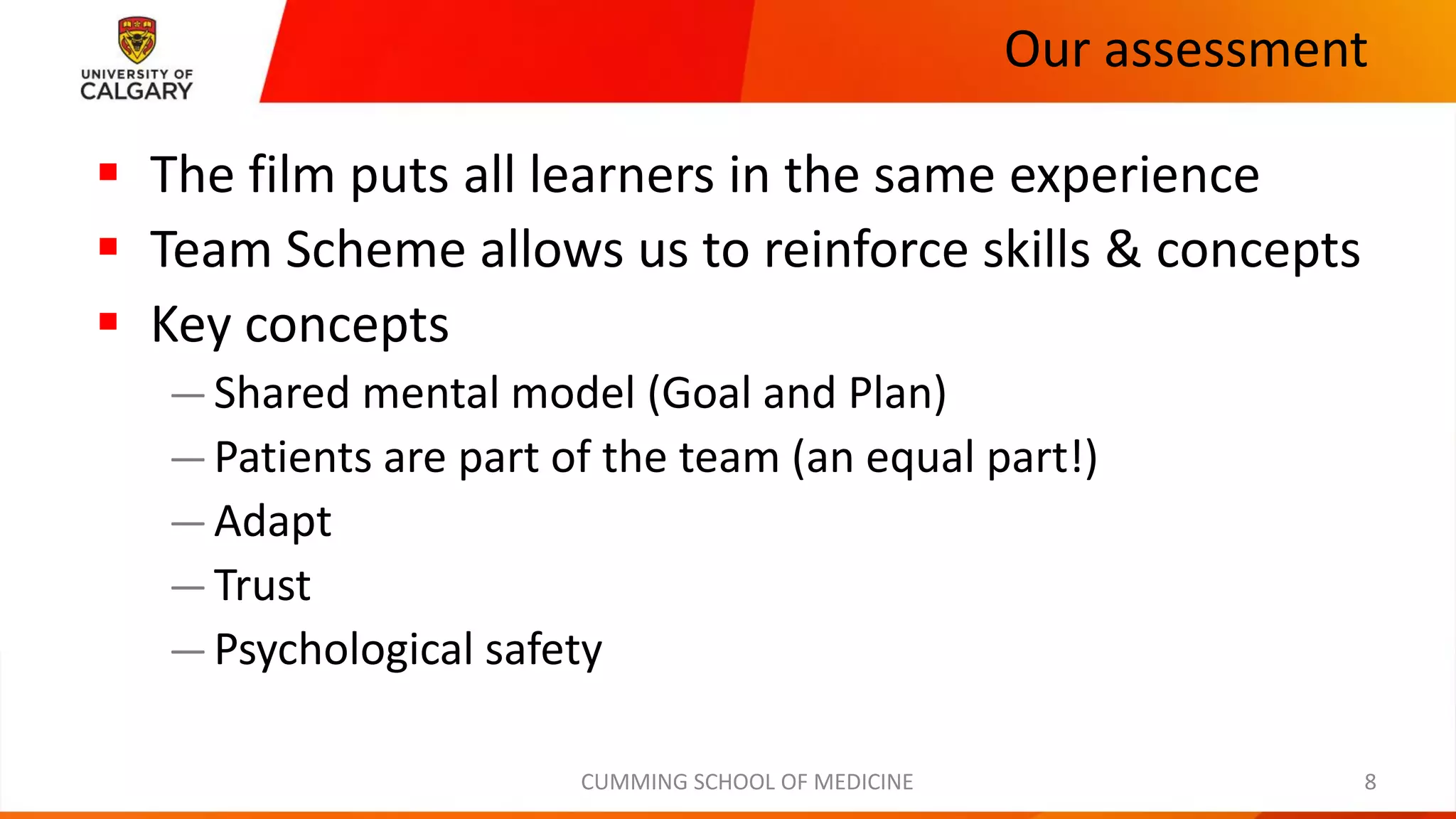
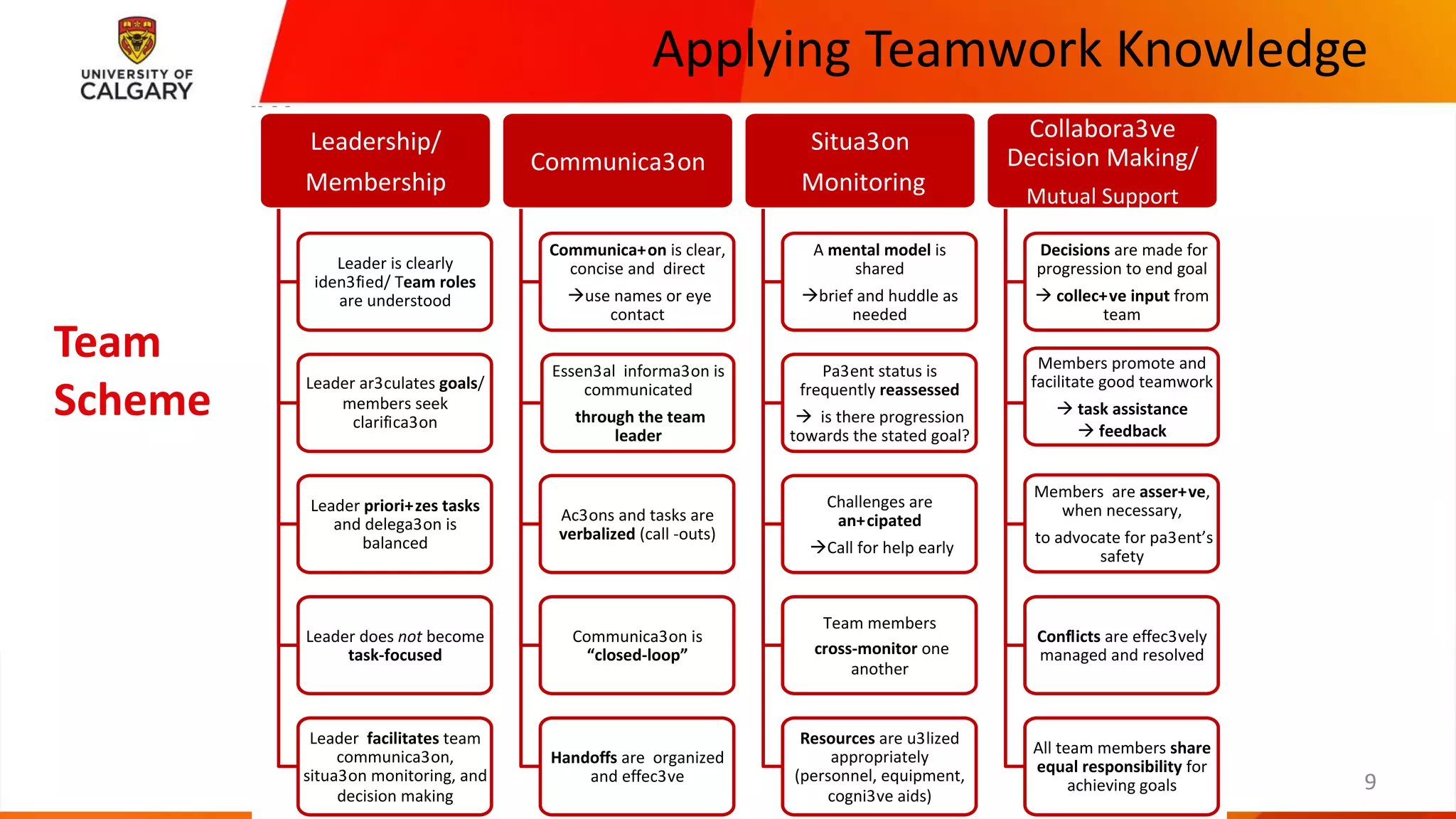



This document discusses teamwork in healthcare and its importance for patient safety. It describes how teamwork skills are often taught through simulations but clinical experience is limited for undergraduates. The intervention described uses a film about a patient falling through the cracks followed by workshops using scenarios to practice and debrief teamwork skills. Key concepts emphasized include shared understanding of goals and plans, involving patients as part of the team, and skills like adaptation, trust, and psychological safety. The overall goal is to apply teamwork knowledge to improve patient outcomes and safety.



































































