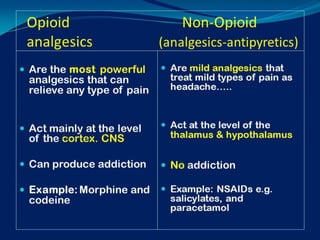
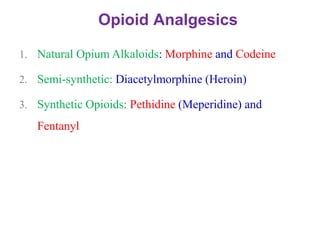
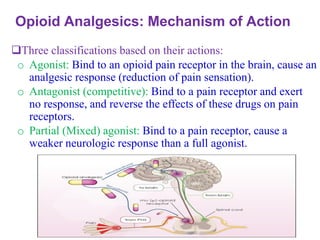
The document provides an overview of analgesic agents affecting the central nervous system, focusing on opioids and non-opioid analgesics, their definitions, mechanisms, indications, contraindications, adverse effects, and nursing implications. Key concepts include physiologic and psychologic dependence, management of opioid toxicity, and considerations for patient education and monitoring. The lecture aims to equip nursing students with comprehensive knowledge of opioid pharmacology and its application in pain management.

![Opioids Analgesics: Psychologic
Dependence
A pattern of compulsive drug use characterized by a
continued craving [desire] for an opioid and the need
to use the opioid for effects other than pain relief.
Opioid tolerance and physical dependence are
expected with long-term opioid treatment and should
not be confused with psychologic dependence
(addiction).](https://image.slidesharecdn.com/topic3-drugsaffectingcns-analgesics-241216155858-63b19fbc/85/Topic-3-Drugs-Affecting-CNS-Analgesics-pdf-15-320.jpg)











![opioids Islamic University [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/opioidsautosaved-250821041508-2c49bca5-thumbnail.jpg?width=640&height=640&fit=bounds)

































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





