Download to read offline



















































![▫ vasodilatation, pain sensitization, gastric
cytoprotection [mucous/HCO3 secretion], fever
▫ bronchoconstriction, uterine contraction
▫ inhibition of platelet aggregation, gastric
cytoprotection
▫ platelet aggregation](https://image.slidesharecdn.com/pharmaday1-221007124803-16f61712/85/Pharma-Day1-pptx-56-320.jpg)



































































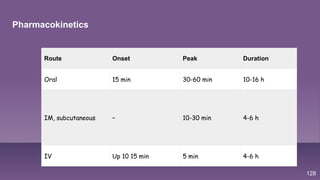

























































This document provides information on opioid analgesics and their use for pain management. It discusses the differences between acute and chronic pain and lists various causes of pain. It then describes different mechanisms for controlling pain, including both non-opioid and opioid options. The rest of the document focuses on opioid analgesics, outlining specific opioid medications, how they work in the body, their indications, contraindications, adverse effects, and considerations for nursing care when administering opioids.