CONTENTS
Introduction
History
Need of Tissueengineering
Triad of Tissue engineering
Strategies of Tissue engineering
Clinical applications
Challenges
Future direction
Conclusion
3.
INTRODUCTION
Tissue engineeringis an emerging field of science aimed at developing techniques
for the fabrication of new tissues to replace damaged tissues and is based on principles
of cell biology, developmental biology and biomaterials science.
The reconstruction of lost tissues or organs has been one of the biggest challenges
posed to all fields of medicine - the reconstruction of the periodontium is no exception.
4.
Tissue engineering, accordingto National Institute of Health definition, is an
emerging multidisciplinary field involving biology, medicine, and engineering
that is likely to revolutionize the way we improve the health and quality of life
for millions of people worldwide by restoring, maintaining, or enhancing tissue
and organ function.
Tissue engineering aims to stimulate the body either to regenerate tissue on its
own or to grow tissue outside the body which can then be implanted as natural
tissue.
DEFINITIONS
5.
HISTORICAL evolution
Uptothe mid -1980’s : The term “tissue engineering” was loosely applied in the literature in
cases of surgical manipulation of tissues and organs or in a broader sense when prosthetic
devices or biomaterials were used.
The term “tissue engineering” as it is nowadays used was introduced in medicine in 1987.
1998- FDA approves Apligraft, first allogenic TE product human embryonic stem cell isolated.
1996- TE society founded TE Regenerative Medicine International Society (TERMIS)
6.
Need for tissueengineering
Tissue engineering holds promise of producing better organs for transplant. Using tissue
engineering techniques & gene therapy it may be possible to correct many otherwise incurable
genetic defects.
A major goal of tissue engineering is in-vitro construction of transplantable vital tissue.
7.
OBJECTIVES
True regenerationof a tissue’s structure and function more predictably, quickly, less
invasively, and more qualitatively.
Promote better healing
8.
Term Tissue engineeringwas originally coined to denote the construction in the laboratory of a
device containing viable cells and biologic mediators in a synthetic or biologic matrix that could
be implanted in patients to facilitate regeneration of particular tissues.
1) Ex vivo- cells can be expanded in culture, attached to a scaffold and then reimplanted into
the host.
2) in vivo- by stimulating the body's own regeneration response with the appropriate
biomaterial.
9.
9
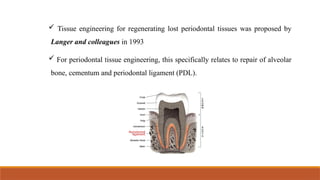
Tissue engineeringfor regenerating lost periodontal tissues was proposed by
Langer and colleagues in 1993
For periodontal tissue engineering, this specifically relates to repair of alveolar
bone, cementum and periodontal ligament (PDL).
10.
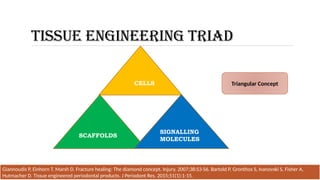
TISSUE ENGINEERING TRIAD
CELLS
SCAFFOLDS
SIGNALLING
MOLECULES
GiannoudisP, Einhorn T, Marsh D. Fracture healing: The diamond concept. Injury. 2007;38:S3-S6. Bartold P, Gronthos S, Ivanovski S, Fisher A,
Hutmacher D. Tissue engineered periodontal products. J Periodont Res. 2015;51(1):1-15.
Triangular Concept
11.
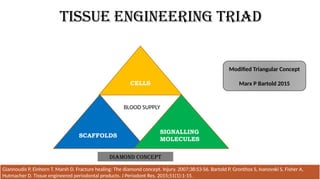
TISSUE ENGINEERING TRIAD
CELLS
SCAFFOLDS
SIGNALLING
MOLECULES
GiannoudisP, Einhorn T, Marsh D. Fracture healing: The diamond concept. Injury. 2007;38:S3-S6. Bartold P, Gronthos S, Ivanovski S, Fisher A,
Hutmacher D. Tissue engineered periodontal products. J Periodont Res. 2015;51(1):1-15.
BLOOD SUPPLY
Modified Triangular Concept
Marx P Bartold 2015
Diamond Concept
12.
Strategies to EngineerTissue
Langer and Vacanti (1993)
Characterised in 3 major classes
Conductive
Inductive
Cell transplantation approaches
13.
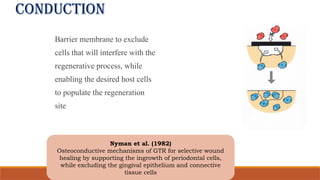
conduction
Barrier membrane toexclude
cells that will interfere with the
regenerative process, while
enabling the desired host cells
to populate the regeneration
site
Nyman et al. (1982)
Osteoconductive mechanisms of GTR for selective wound
healing by supporting the ingrowth of periodontal cells,
while excluding the gingival epithelium and connective
tissue cells
14.
INDUCTION
‡Activating cells inclose
proximity to the defect site with
specific biological signals
‡Origins of this mechanism
are rooted in bone morphogenetic
proteins
Urist et al. (1965)
New bone could be formed at ectopic sites after implantation
with powdered bone containing BMPs which are the key
elements for inducing bone formation.
15.
Cell transplantation
‡Involves directtransplantation
of cells grown in the laboratory
‡It truly reflects the multidisciplinary
nature of tissue engineering, as it
requires the clinician or surgeon, the
bioengineer, and the cell biologist
16.
TISSUE ENGINEERING TRIAD
CELLS
Regeneration of lost tissues shall require the recruitment of cells that have the potential to
differentiate into specialized regenerative cells
The cell types for periodontal healing include:
Sources
Autologous Cells
Allogenic Cells
Xenogenic Cells
Stem Cells
17.
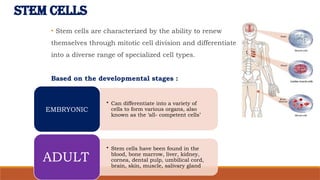
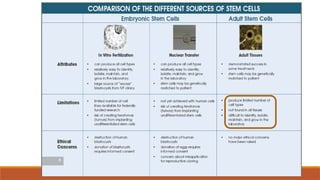
STEM CELLS
• Stemcells are characterized by the ability to renew
themselves through mitotic cell division and differentiate
into a diverse range of specialized cell types.
Based on the developmental stages :
• Can differentiate into a variety of
cells to form various organs, also
known as the ‘all- competent cells’
EMBRYONIC
• Stem cells have been found in the
blood, bone marrow, liver, kidney,
cornea, dental pulp, umbilical cord,
brain, skin, muscle, salivary gland
ADULT
19.
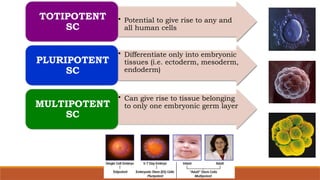
• Potential togive rise to any and
all human cells
TOTIPOTENT
SC
• Differentiate only into embryonic
tissues (i.e. ectoderm, mesoderm,
endoderm)
PLURIPOTENT
SC
• Can give rise to tissue belonging
to only one embryonic germ layer
MULTIPOTENT
SC
20.
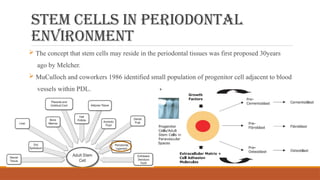
Stem cells inperiodontal
environment
The concept that stem cells may reside in the periodontal tissues was first proposed 30years
ago by Melcher.
MuCulloch and coworkers 1986 identified small population of progenitor cell adjacent to blood
vessels within PDL.
21.
SIGNALLING MOLECULES
Oneof the most physiologically efficient methods for stimulating cells is the
use of cytokines or growth factors.
Some researchers have attempted to accelerate the regeneration of periodontal
tissue by using topical application of human recombinant cytokines to
stimulate proliferation and differentiation of the undifferentiated
mesenchymal cells into cells that form hard tissues, such as osteoblasts and
cementoblasts.
22.
SEMIPURIFIED
PREPARATIONS
Autologous platelet-rich plasma
preparations
Enamelmatrix derivative
RECOMBINANT GROWTH
FACTORS
• Recombinant human platelet-
derived growth factor-BB
• Recombinant human basic
fibroblast growth factor
• Morphogens such as
recombinant human bone
morphogenetic protein
Two basic approaches….
23.
Proteins thatmay act locally or systemically to affect the growth and function of cells in
various manners.
3 functions:
1. Mitogenic (proliferative)
2. Chemotactic (stimulate directed migration of cells)
3. Angiogenic (stimulate new blood vessel formation) effects
24.
The rate ofgrowth factor release depends
◦ Rate of degradation
◦ Rate of growth factor diffusion through pores of the scaffolds.
Several bioactive molecules have been demonstrated like PDGF, IGF-I, basic fibroblast
growth factor (FGF-2) , TGF-1, BMP-2, -4, -7 and -12, and have shown positive results
in stimulating periodontal regeneration.
25.
BONE MORPHOGENIC PROTEINS(BMP)
The most remarkable feature of BMPs is the ability to induce ectopic bone
formation.
Multifunctional growth factors belonging to the TGF-β superfamily.
Osteoinductive properties.
Now available in recombinant forms
The primary action of BMPs is to differentiate mesenchymal precursor cells into cartilage and bone-
forming cells.
Up-regulating the angiogenetic peptides like VEGF.
26.
BMP-2
• Differentiation of
osteoblasts
•BMPs 5, 6 and 7
augment BMP-2
BMP-3
(osteogenin)
• Induces cartilage
formation
BMPs 2, 4 and 7
• Recombinant
BMPs 2 and 4
used as a
substitute for
dental epithelium
in inducing
mesenchyme
differentiation
BMP 3 and BMP 7
• have been
immunolocalized
to developing
PDL, cementum
and alveolar
bone.
27.
FIBROBLAST GROWTH FACTORFAMILY
Heparin binding growth factor family
7 forms (2 described) :
• FGF 1 acidic(aFGF)
• FGF 2 basic (bFGF)
FGF-2 is more potent.
Function: Mitogen & chemoattractant.
Stimulate proliferation of osteogenic cells and enhance matrix production
28.
PLATELET-DERIVED GROWTH FACTOR
Secretedfrom platelets & subsequently by macrophages.
‡Effect on osteoblasts
Stimulates mitogenic and chemotaxis in Osteoblast
Osteoblast have numerous PDGF receptors
(Canalis et al.1989, Kilian et al. 2004)
‡Effect on PDL cells
PDGF enhanced proliferation of pdl cells both
with osteoblastic and fibroblastic phenotype
(Piche et al. 1989,Camargo et al. 2002)
29.
INSULIN-LIKE GROWTH FACTORS
Peptidegrowth factors with biochemical & functional similarities to insulin.
Bone cells produce & respond to IGF’s, and bone is a storage house for these factors in their
inactive form.
Effect on PDL cells and osteoblasts
‡Stimulate bone formation, bone matrix formation
‡Improves adhesion of cells to root surface
‡Acts synergistically with PDGF- a chemotactic for PDL cells
‡Stimulates mitogenic activity
30.
SCAFFOLDS
Porous three-dimensionaltemporary scaffolds play an important role in
manipulating cell function and guidance of new organ formation.
Replicate native ECM
Provide a cell-adhesion substrate
31.
DESIGN CRITERIA
Shouldpermit cell adhesion, promote cell growth, and allow the retention of differentiated cell
functions.
Should be biocompatible, neither the polymer nor its degradation by-products should provoke
inflammation or toxicity.
Should be biodegradable and eventually eliminated.
The porosity should be high enough to provide sufficient space for cell adhesion, extracellular
matrix regeneration.
32.
Hyaluronic Acid, Alginate,Agarose, Albumin, Chitosan, Collagen,
Glycosaminoglycans (GAGS).
Advantages: Low toxicity & lower chronic inflammatory response.
Disadvantages: Poor mechanical strength as well as a complex structure and,
hence, manipulation becomes more difficult.
Examples of Natural materials
33.
COLLAGEN
Fibrous proteinwith a long, stiff, triple-stranded helical structure.
Most abundant and ubiquitous structural protein in the body
Readily purified from both animal and human tissues with enzyme treatment
and salt/ acid extraction.
Assist to retain the phenotype and activity of many types of cells, including
fibroblasts and chondrocytes.
33
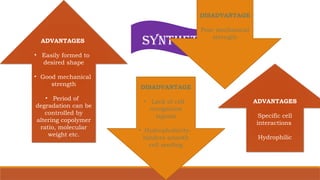
NATURAL
ADVANTAGES
• Easily formedto
desired shape
• Good mechanical
strength
• Period of
degradation can be
controlled by
altering copolymer
ratio, molecular
weight etc.
DISADVANTAGE
• Lack of cell
recognition
signals
• Hydrophobicity-
hinders smooth
cell seeding
SYNTHETIC
DISADVANTAGE
Poor mechanical
strength
ADVANTAGES
Specific cell
interactions
Hydrophilic
36.
Hybrid scaffolds
PLGA sponge+ collagen sponge
Hybridization with collagen improved the wettability of synthetic sponges with water, which
facilitated cell seeding.
Possessed almost the same high degree of mechanical strength as those of synthetic
polymers, much higher than that of collagen sponges alone.
Should be osteoconductive so that osteoblasts and osteoprogenitor cells can adhere, migrate,
differentiate, and synthesize new bone matrix.
Hydroxyapatite has a composition and a structure very close to natural bone mineral and is,
thus frequently used as hybrid scaffolds in bone tissue engineering.
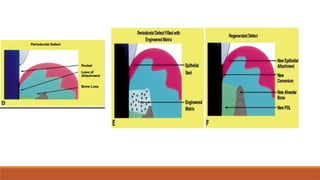
Criteria must metin order for
periodontal regeneration
1. Functional epithelial seal must be re-established at the coronal most portion of the
tissues.
2. New CT fibres must be inserted into the previously exposed root surface to
reproduce both pdl and dentogingival fibre complex
3. New, acellular, extrinsic fibre cementum must be reformed on the previously
exposed root surface.
4. Alveolar bone height must be restored to within 2mm of the CEJ
39.
GUIDED TISSUE REGERATION
Nyman and Karring in the 1982 proposed the use of GTR
for periodontal regeneration.
Marked the evolution of periodontal regeneration technologies
using tissue engineering.
Used alone or in combination with regenerating material
Properties:
• Space provision
• Epithelial cell occlusion
• Exclusion of gingival connective tissue & selective
repopulation of periodontal ligament cells on root surface.
39
40.
Enamel matrix proteins
Biologybased therapy
‡Play an important role in tooth development
‡Secreted by the Hertwig’s epithelial root sheath – contribute not only to
cementogenesis but also in the development of periodontal attachment
apparatus.
Hammartsrom et al., 1997
41.
EMD promotes arange of cell activities: Sculean et al. (2007)
The proliferation and growth of PDL fibroblasts
Inhibiting proliferation of epithelial cells;
Increased total protein synthesis of the PDL fibroblasts;
The formation of mineralized nodules by PDL fibroblasts;
The growth of mesenchymal cells;
The release of autocrine GFs from PDL fibroblasts
‡EMD-stimulated expression of BMPs from macrophages might induce
cementum-like material from cells like fibroblasts
Fujishiro et al. (2008)
42.
RECOMBINANT PROTEIN DERIVATIVES
Synthesized purified proteins packaged in large sterile
quantities.
To date, only three recombinant growth factor products have
been widely used
1. rh PDGF-BB (gel)
2. rhPDGF-BB (with β tricalcium phosphate)/GEM 21S
3. rh BMP-2 (with type I collagen sponge)
42
43.
Title, Author MethodResult Conclusion
Intrabony Defects
Management Using Growth
Factor
Enhanced Matrix versus
Platelet Rich Fibrin Utilizing
Minimally Invasive Surgical
Technique: A Randomized
Control Study.
Raslan et al, 2021
Journal of Research in Medical
and Dental Science
21 intra-bony defects in fifteen
patients with moderate to
severe
periodontitis were randomly
classified into 3 groups, 7 sites
each. Group І treated by MIST
alone, group ІІ treated by
MIST
+ EDTA + PRF group III treated
by MIST+EDTA+GEM 21S
CBCT analysis showed
statistically significant
improvement in bone level 9
months. group III showed the
best improvement followed by
group II and
group I.
The
adjunctive use of GEM 21S
provided superior benefits on
the outcome of MIST for the
treatment of intra-bony
defects.
CELL SHEET ENGINEERING
•Cell sheet technology enables novel approaches to tissue engineering without
the use of biodegradable scaffolds.
• To avoid enzymatic degradation, a new culture surface was invented using poly N-
isopropylacylamide.
• This surface allows harvesting of intact cell sheets through low temperature treatment.
• This continuous cell sheet preserves an intact extracellular matrix and normal cell functions.
46.
‡ PDL cellsare harvested on thermo-responsive culture dishes [UpCell™
(CellSeed Inc., Tokyo, Japan)] in the presence of ascorbic acid, producing
intact periodontal cell sheets with thick extracellular matrix(ECM)
‡ Fibronectin is a major protein incorporated into the ECM, which
functions as a natural adhesive to attach cell sheet to other surfaces.
48.
GENE THERAPY
Gene therapyis defined as the treatment of disease or disorder by transferring
genetic materials, to introduce, suppress, or manipulate specific genes that
direct an individual’s own cells to produce a therapeutic agent.
Targeting cells for gene therapy requires the use of vectors or direct delivery
methods to transfect them.
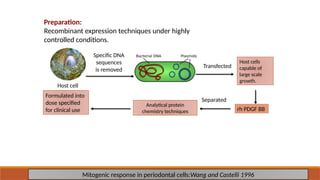
Preparation:
Recombinant expression techniquesunder highly
controlled conditions.
Mitogenic response in periodontal cells:Wang and Castelli 1996
Specific DNA
sequences
is removed
Transfected
Host cells
capable of
large scale
growth.
rh PDGF BB
Separated
Analytical protein
chemistry techniques
Formulated into
dose specified
for clinical use
Host cell
50
51.
Challenges in stemcell based
research to practice
BIOLOGIC TECHNICAL CLINICAL
52.
BIOLOGICAL CHALLENGES
Notall findings in animals model can be directly applied to humans.
The molecular pathway that underlie stem cell self- renewal and differentiation are also largely
unknown.
Complete and predictable regeneration still
remains an elusive clinical goal
53.
TECHNICAL CHALLENGES
‡Associated withcell manipulations, scaffold materials and delivery systems.
‡Culture conditions are not sufficiently developed to mimic the cell
microenvironment in vivo.
‡Timing is an inherent constraint. Some involve weeks to months of ex vivo
processing.
‡Search for the ideal biocompatible scaffolding material(s) and delivery system.
Attila Horváth intheir study on Novel Technique to Reconstruct Peri-Implant Keratinised
Mucosa Width Using Xenogeneic Dermal Matrix. Clinical Case Series concluded that
After split thickness flap preparation, the XDM was trimmed, rehydrated and tightly attached to
the recipient periosteal bed using modified internal/external horizontal periosteal mattress
sutures via secondary wound healing. Change of the peri-implant keratinised mucosa width
(PIKM-W) and dimension of the graft remodelling were evaluated at 6 and 12 months
postoperatively.
Clinical parameters showed statistically significant intra- and intergroup differences between the
baseline and 6 and 12 months (p < 0.05). The present technique using the XDM was safe and
successfully reconstructed PIKM-W in both arches. The XDM alone seems to be a suitable
alternative to autograft for PIKM-W augmentation in the maxilla
56.
Conclusion
The challengein regenerative periodontal therapy lie in the ability to induce the regeneration
of a complex apparatus.
There is need for novel regenerative technologies to be developed based on contemporary
understanding.
With the application of tissue engineering principles, it now seems that complete periodontal
regeneration may be possible but further long term studies are required…
57.
REFERENCES
• Yoshida T,Washio K, Iwata T, Okano T, Ishikawa I.
Current status and future development of cell transplantation therapy for periodontal tissue rege
neration. Int J Dent 2012;1-8
• Pandit N, Malik R, Philips D. Tissue engineering: A new vista in periodontal regeneration. J
Indian Soc Periodontol 2011;15(4):328-37.
• Izumi Y, Aoki A, Yamada Y, Kobayashi H, Iwata T, Akizuki T, et al.
Current and future periodontal tissue engineering. Periodontol 2000 2011;56:166-87
58.
• Du M,Duan X, Yang P. Induced Pluripotent Stem Cells and Periodontal Regeneration. Curr Oral
Health Rep. 2015;2(4):257-265.
• Baydik OD, Titarenko MA, Sysolyatin PG. Tissue engineering in dentistry. Stomatologiia (Mosk).
2015;94(2):65-8.
• Bartold PM. Group C. Initiator paper. Periodontal regeneration--fact or fiction? J Int Acad Periodontol.
2015 :17(1 Suppl):37-49.
• Jin LJ, Zhang C. Periodontal ligament stem cells: an update and perspectives. J Investig Clin Dent.
2014 ;5(2):81-90.
• Rasperini G, Pilipchuk SP, Flanagan CL, Park CH, Pagni G, Hollister SJ, Giannobile WV. 3D-printed
Bioresorbable Scaffold for Periodontal Repair. J Dent Res. 2015 Sep;94(9 Suppl):153S-7S.
• Horváth, A.;Windisch, P.; Palkovics, D.; Li, X. Novel Technique to Reconstruct Peri-Implant Keratinised
MucosaWidth Using Xenogeneic Dermal Matrix. Clinical Case Series. Dent. J. 2024, 12, 43.
https://doi.org/10.3390/dj12030043
Editor's Notes
#3 Interdisiplinarly field which applies the principles of engg and life science tools
#50 They are first produced by removing the specific DNA sequences from a human cell and transfecting it into a bacterial plasmid. The bacterial plasmid is then
transfected into the host cells capable of large scale growth. These are essentially protein factories that synthesize and secrete many proteins. The rh PDGF BB is then separated using sophisticated analytical protein chemistry techniques, sterile filtered and formulated into dose specified for clinical use



![‡ PDL cells are harvested on thermo-responsive culture dishes [UpCell™
(CellSeed Inc., Tokyo, Japan)] in the presence of ascorbic acid, producing
intact periodontal cell sheets with thick extracellular matrix(ECM)
‡ Fibronectin is a major protein incorporated into the ECM, which
functions as a natural adhesive to attach cell sheet to other surfaces.](https://image.slidesharecdn.com/tissueeng-250314015456-5eae3a2a/85/tissue-engeneering-in-periodontics-pptxmn-46-320.jpg)