Reference Guidelines
• TheInvestigation and Treatment of Couples with
Recurrent First trimester and Second-trimester
Miscarriage. RCOG Green-top Guideline No. 17,
2011
• Evaluation and Treatment of Recurrent Pregnancy
Loss. Practice committee of American Society of
Reproductive medicine (ASRM). 2012
• Evidence-based guidelines for the investigation and
medical treatment of recurrent miscarriage. ESHRE
Campus workshop. 2006
4.
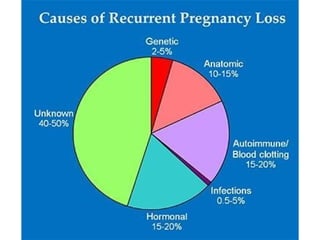
Disease Burden
• 15%of clinically recognized pregnancies result
in
pregnancy failure
• 5% of couples trying to conceive have 2 consecutive
losses
• 1% of couples trying to conceive have 3 consecutive
losses
• Only 30% of all conceptions result in a live birth
Stirrat et al. Lancet 1990;336:673–5
Wyatt et al. Am J Obstet Gynecol 2005;192:240–6
5.
Case 1
• 32years old lady, P0A2
• History of 2 prior first trimester
spontaneous abortions (USG proven-missed
abortion)
• Presents for work up of pregnancy losses
Should you label her as a case of RPL and
start work up?
6.
Definition
• Recurrent miscarriageis defined as two or
more pregnancy loss
-ASRM, 2012
• RPL is defined as the loss of three or
more consecutive pregnancies.
-NICE guidelines, 2011
• Initiation of evaluation appropriate after
2 losses based on patient age and desire
-NICE guidelines, 2011; ESHRE guidelines, 2006
7.
Case 2
• 36years old lady, P0A2
• History of 2 prior first trimester
spontaneous abortions (USG proven)
• Wants to know the chances of again having
an abortion
How should you counsel her about future
risks?
Risk Factors
• MaternalAge≥35 years
35–39 years-25%
40–44 years-51%
miscarriages (40% after 3
• Number of
previous consecutive
losses)
• Paternal age ≥40 years
•
Maternal cigarette smoking, caffeine
consumption, heavy alcohol consumption (Dose
dependent)
• Obesity & Stress increases risk of sporadic and recurrent
miscarriage
12.
Case 3
• 28year old lady, P0 A3
• History of three first trimester abortions
(USG proven, no records)
• No other significant history
• Comes to you for work up
How will you work her up?
14.
History Taking
• Age,previous pregnancies, weeks at miscarriage, any
problems during pregnancy like preeclampsia &
FGR
• Family history of miscarriages, pre-
eclampsia, diabetes, VTE and thrombophilias
• Habits: smoking, coffee, alcohol, workplace and stress
levels
• Medications including natural supplements
• Review of systems for bloating, diarrhea, mucus
in
stool, floating stool, joint pain, rashes,
polydipsia,
polyuria, nocturia, fatigue, cold
intolerance,
palpitations, thyroid masses
16.
Battery of Investigations
•CompleteBlood Count
•Pelvic ultrasound scan
•Thyroid Function Test
•OGTT
•Antiphospholipid
antibodies (LA, IgG and IgM
ACA)
•Embryonic tissue
karyotype
•Factor V leiden, PT gene
mutation, protein C & S, AT
III, factor VIII, MTHFR,
homocysteine
•Thyroid antibodies
•LH, FSH, Prolactin,
progesterone
•Parental karyotype
•ANA, RF, anti-TTG
•Vaginal/cervical cultures,
Hep B/C, HIV, Parvovirus,
Syphillis
17.
Case 4
• 28year old lady, P1L0 A3
• History of preeclampsia & preterm induced
delivery at 29 weeks, baby expired on day 9.
• History of three first trimester abortions
(USG showed cardiac activity)
What seems to be the likely cause of recurrent
pregnancy loss?
18.
Anti-phospholipid Syndrome
• Mostimportant treatable cause of
recurrent
miscarriage
• Antiphospholipid syndrome refers to the
between
–
antiphospholipid
anticoagulant,
lupus
antibodies
association
antibodies
anticardiolipi
n
glycoprotein-I
antibodies –
and anti-B2
and
adverse
pregnancy outcome or vascular thrombosis.
NICE guidelines on RPL, 2011
19.
APLA (Disease Burden)
•APL antibodies present in 15% of
women
with recurrent miscarriage
• Prevalence of APL antibodies in women with
a low-risk obstetric history - <2%
• Live birth rate in pregnancies with
APLA
without intervention -10%
Human Reprod 1995;10:2001–5
Hum Reprod 1995;10:3301–4.
20.
How APLA causepregnancy morbidity?
• Activation
of
complement
pathways
at the
maternal–fetal interface resulting in a local
function and
inflammatory response
• Inhibition of
trophoblastic
differentiation
• In later pregnancy, thrombosis of the uteroplacental
vasculature
In vitro studies have shown that effect of APL antibodies on
trophoblast function and complement activation is reversed by
heparin
Laboratory Diagnosis ofAPLA
Two positive tests at least 12 weeks apart for-
• Lupus anticoagulant (dilute Russell’s viper
venom time test with platelet neutralisation
procedure is more sensitive and specific than
either aPTT test or Kaolin Clotting Test)
or
• Anticardiolipin IgG / IgM (> 40 g/l or > 99th
percentile) by ELIZA
24.
Treatment of APLA
•Low-dose aspirin plus heparin in pregnancy
• LMW heparin is as safe as
unfractionated heparin
• Potentia
l
advantages i.e. less heparin-
induced thrombocytopenia, once daily dosing
and lower risk of heparin-induced
osteoporosis
25.
Therapeutic Management ofAPS Pregnancies
Clinical History Anticoagulant therapy
No thrombosis, no miscarriage, no
adverse pregnancy outcome
Aspirin 75 mg o.d. from pre-conception
Previous thrombosis On maintenance warfarin: transfer to aspirin
and LMWH (enoxaparin 40 mg b.d.) as soon
as pregnancy confirmed
Not on warfarin: aspirin 75 mg o.d. from
preconception and commence LMWH
(enoxaparin 40 mg o.d.) once pregnancy
confirmed.
Increase LMWH to bd at 16-20 weeks
26.
Therapeutic management ofAPS pregnancies
Clinical History Anticoagulant therapy
Recurrent miscarriage <10 weeks No prior anticoagulant therapy: Aspirin 75
mg o.d. from pre-conception
Prior miscarriage with aspirin alone: Aspirin
75 mg o.d. from pre-conception and LMWH
(enoxaparin 40 mg o.d.) once pregnancy
confirmed.
Consider discontinuation of LWWH at 20
weeks' gestation if uterine artery waveform
is normal
Late fetal loss, neonatal death or
adverse outcome due to pre-
eclampsia, IUGR or abruption
Aspirin 75 mg o.d. from pre-conception and
LMWH (enoxaparin 40 mg o.d.) once
pregnancy confirmed
27.
Case 5
• 28year old lady, P1L0 A3
• History of preeclampsia and preterm delivery at
29 weeks, baby expired on day 9.
• History of three abortions
• History of DVT and stroke in first degree
relatives
What seems to be the likely cause of
recurrent
pregnancy loss?
Thrombophilias
• Both inheritedand acquired thrombophilias
lead to RPL
– Activated protein C resistance
– Factor V Leiden mutation
– Deficiencies of protein C/S
– Deficiencies of antithrombin III
– MTHFR gene defect
– Prothrombin gene mutation
– Hyperhomocysteinaemia
30.
Thrombophilia Testing
Women withrecurrent second trimester
miscarriages should be screened for
inherited thrombophilias including
factor V Leiden, factor II (prothrombin)
gene mutation and Protein S
NICE guidelines on RPL, 2011
31.
Role of Heparinin Inherited Thrombophilia
• Insufficient evidence to evaluate the effect of
heparin to prevent miscarriage with
recurrent first-trimester miscarriage
• Heparin therapy beneficial in improving live
birth rate of women with second-trimester
miscarriage
• Heparin therapy in history of thrombosis
is
beneficial
32.
Case 6
• 31years old lady, P0 A3
• History of three second trimester
abortions at 20 and 23 weeks
What seems to be the likely cause of recurrent
pregnancy loss?
Role of SeptumResection
There is insufficient evidence to assess
the effect of uterine septum resection in
women with recurrent miscarriage and
uterine septum to prevent further
miscarriage
ASRM guidelines, 2012
35.
Anatomical Causes
• Prevalenceof uterine malformations higher in
second-trimester miscarriages as compared to first-
trimester miscarriages
• May be related to the cervical weakness
•
•
Arcuate uteri –
Septate uteri
–
Risk of second trimester abortion
Risk of first trimester abortion
Hum Reprod 2003;18:162–6.
36.
Anatomical
Factors
All women withrecurrent first-trimester
miscarriage and all women with one or
more second-trimester miscarriages
should have a pelvic ultrasound to
assess uterine anatomy
NICE guidelines on RPL, 2011
37.
Case 7
• 31years old lady, G4P1L0A2 at 20
weeks
gestation
• History of preterm delivery at 28
weeks
(delivery within 1/2 hour of pain)
• History of two second trimester abortions at
22 and 24 weeks
What seems to be the likely cause of recurrent
pregnancy loss?
Role of Cerclage
•History of second-trimester miscarriage and
suspected cervical weakness may be offered serial
sonographic surveillance
• An ultrasound-indicated cerclage should be offered
if cervical length < 25mm is detected by TVS before
24 weeks gestation
• Cerclage should be offered to women with previous
three preterm deliveries/second trimester abortion
ACOG guidelines, 2012
40.
Case 8
• 35years old lady, P0 A2
• History of prolonged cycles
• History of three abortions
• BMI-31 kg/m2;
• Waist/Hip ratio- 1.1 (Apple Shaped Woman)
• Examination reveals dark patch on nape of neck (AN)
What seems to be the likely cause of recurrent
pregnancy loss?
Endocrine Causes
• Diabetesmellitus (with high
1st
trimester HbA1C)
and uncontrolled thyroid disease (with anti-thyroid
antibodies) have been associated with miscarriage
• Well-controlled diabetes mellitus & treated thyroid
dysfunction is not a risk
• PCOS (Increased risk due to insulin
resistance, hyperinsulinaemia &
hyperandrogenaemia)
• Luteal phase deficiency, hyperprolactinemia
Diabetologia 1990;33:100–4
43.
Case 9
• 26years old lady, P0 A4
• History of 4 first trimester abortions
• History of diarrhea, steatorrhea, weight loss,
bloating, flatulence, abdominal pain
What seems to be the likely cause of recurrent
pregnancy loss?
Immunological Causes
• Untreatedceliac disease has been associated
• Modest associations between cytokine
polymorphisms and recurrent miscarriage
• Further research is required before routine
cytokine tests can be introduced to clinical
practice.
NICE guidelines on RPL, 2011
47.
Case 10
• A32 years old lady G4A3, reports to Gynae
casuality at 13 weeks gestation with
inevitable abortion
• She has been worked up earlier and her
blood investigations for RPL are normal
• What will you do next?
48.
Genetic Causes
• Cytogeneticanalysis to be performed on
products of conception of RPL patient
• Parental peripheral blood karyotyping of
both partners should be performed
where
testing of products of conception reports
chromosomal
Balanced structural
abnormality
NICE guidelines on RPL, 2011
50.
What to doif genetic defect diagnosed?
• Prompt referral to a clinical geneticis
• Prognosis for risk of future pregnancies and opportunity
for
familial chromosome studies
• Reproductive options include natural pregnancy with or
without a prenatal diagnosis test, gamete donation and
adoption
• Preimplantation genetic diagnosis is a treatment option
for
translocation carriers
• Preimplantation genetic screening with IVF treatment in
improve live birth rates NICE guidelines on RPL, 2011
51.
Role of Infections
•Severe infection that leads to bacteraemia or viraemia can
cause sporadic miscarriage.
• Role in recurrent miscarriage is unclear
• Routine TORCH screening should be abandoned
• Bacterial vaginosis in second trimester can cause second-
trimester miscarriage
• Chronic infection in immuno-compromized patients
may cause RPL
• Mycoplasma, Ureaplasma, Chlamydia,
Listeria
monocytogenes & HSV has some role
NICE guidelines on RPL, 2011
52.
Male Factor
• Abnormalsperm quality has been associated
with recurrent pregnancy losses
• Role is controvercial
• Testing not recommended
53.
Management of UnexplainedRPL
• Aspirin + heparin usage in unexplained RPL is
controversial
• Use of empirical treatment in women with
unexplained recurrent miscarriage is
unnecessary
• Excellent prognosis without pharmacological
intervention if offered supportive care in a
dedicated early pregnancy assessment unit
NICE guidelines, 2012
54.
Management of UnexplainedRPL
• Folic acid supplementation is recommended
• Role of Progesterones – Controversial;
Recent large trial shows no role*(PROMISE
Trial)
• Insufficient evidence to evaluate the
effect of
HCG supplementation
• Insufficient evidence to evaluate effect of
metformin supplementation
*Coomarasamy A et al. A Randomized Trial of Progesterone in Women with
Recurrent Miscarriages. N Eng J Med 2015 Nov 26;373(22)
Summary
• RPL isdefined as 3 consecutive pregnancy
losses
prior to 24 weeks
• Role of evaluation after 2 losses is acceptable
• Proven etiologies include parental chromosomal
abnormalities, untreated
hypothyroidism, uncontrolled diabetes, uterine
anamolies, and antiphospholipid antibody
syndrome (APS).
57.
• Possible etiologiesinclude other endocrine disorders,
thrombophilias, immunologic abnormalities, and
environmental causes
• More than 33% of all cases will remain unexplained
• Diagnostic evaluation & therapy directed towards any
treatable etiology
• Antenatal counseling and psychological support
should be offered
Summary


























































































![MDR_1st_Dec_2025[1].pptx maternal mortality](https://cdn.slidesharecdn.com/ss_thumbnails/mdr1stdec20251-251203175305-40cf031e-thumbnail.jpg?width=640&height=640&fit=bounds)
![MDR_1st_Dec_2025[1] Final.pptx maternal mortality](https://cdn.slidesharecdn.com/ss_thumbnails/mdr1stdec20251final-251203175141-4e224fe5-thumbnail.jpg?width=640&height=640&fit=bounds)