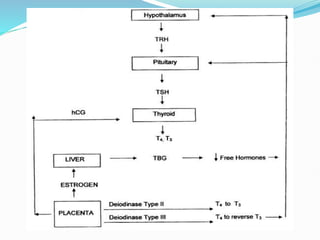
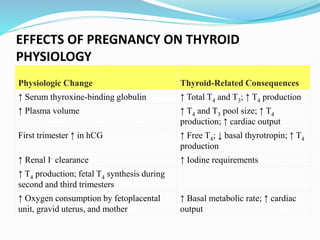
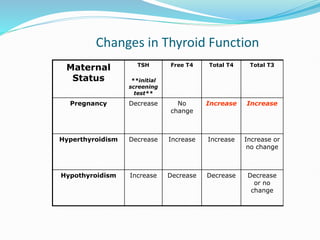
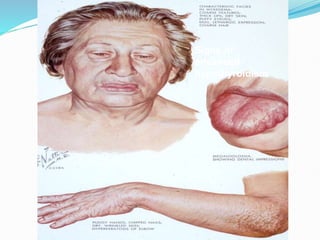
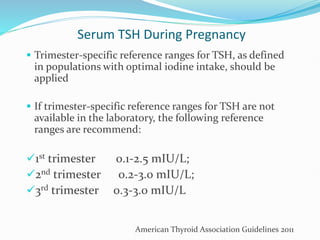
The document discusses the effects of pregnancy on thyroid physiology and function. It notes that pregnancy causes increases in thyroid binding globulins, plasma volume, hCG levels, and iodine requirements, all of which impact thyroid hormone levels. It also discusses the prevalence and causes of hypothyroidism in pregnancy, signs and symptoms, effects on maternal and fetal outcomes, and treatment recommendations including levothyroxine dosage optimization during pregnancy.














































![Dysbiosis & Probiotics Gyn Final (1) [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dysbiosisprobioticsgynfinal1autosaved-230702143604-d104eddc-thumbnail.jpg?width=640&height=640&fit=bounds)






















