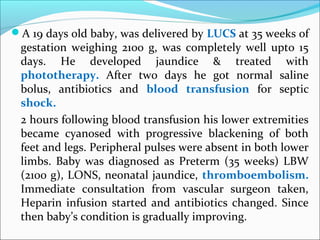
1. A 19 days old baby, was delivered by LUCS at 35 weeks of
gestation weighing 2100 g, was completely well upto 15
days. He developed jaundice & treated with
phototherapy. After two days he got normal saline
bolus, antibiotics and blood transfusion for septic
shock.
2 hours following blood transfusion his lower extremities
became cyanosed with progressive blackening of both
feet and legs. Peripheral pulses were absent in both lower
limbs. Baby was diagnosed as Preterm (35 weeks) LBW
(2100 g), LONS, neonatal jaundice, thromboembolism.
Immediate consultation from vascular surgeon taken,
Heparin infusion started and antibiotics changed. Since
then baby’s condition is gradually improving.
2.
3.
4.
5.
6. Thromboembolism in newborn
Dr. Md Hanif Sumon
Resident (Phase-A)
Dept. of Neonatology
BSMMU
Dr. Md. Shameem
Resident (Phase-B)
Dept. of Neonatology
BSMMU
7. Normal haemostatic mechanism
There are four phases
to the normal
coagulation cascade:
Blood vessel
constriction
Platelet aggregation
Fibrin generation
Vessel repair and
fibrin degradation
8. Basic steps of blood coagulation
3 Basic steps of blood coagulation:
Step-1 :Generation of prothrombin activator(Factor-x) by
extrensic or intrinsic pathway.
Step-2: Conversion of prothrombin to thrombin by
prothrombin activator.
Step-3: Conversion of fibrinogen to fibrin(clot) by thrombin.
9. Intrinsic clotting system
The intrinsic clotting
pathway requires at least
four coagulation proteins
and two co-factors.
Tested using the aPTT.
10. Activation of intrinsic pathway
The intrinsic pathway is
initiated by the exposure
of blood to a negatively
charged surface and
activation of Factor XII.
11. Extrinsic clotting system
The extrinsic system, in
contrast, requires only one
coagulation protein and two
co-factors (Ca & TF ).
Extrinsic pathway is assed
with PT.
12. Activation of extrinsic pathway
Tissue thromboplastin
(tissue factor) is present on
the surface of perivascular
tissue cells but is only
exposed to blood flow
during injury.
Thromboplastin, in the
presence of calcium, binds to
Factor VII to cause the
activation of Factor X.
18. Pathophysiology
Thrombus is a solid mass formed in the circulation from the
constitution of the blood during life. It is composed of :
Fibrin
Platelets
Red cells
Fate of thrombus:
Propagation : complete obstruction
Embolization
Dissolution by fibrinolytic activity
Organization and recanalization
Embolus
Any intravascular solid, liquid or gaseous mass carried by the
blood to a site distant from its point of origin.
99% arise from thrombi, so the term thromboembolism.
20. Hemostatic system of neonate
Hemorrhage > thrombosis
The vascular endothelium system has not accumulated
damage from disease or acquired factor.
Levels of vitamin K related clotting factor are low.
Antithrombin, protein C, protein S levels are low.
Decreased fibrinolytic potential.
21. Epidemiology
Thrombosis occurs more frequently in the neonatal period than
at any other age in childhood.
2.4 per 1,000 admissions to the NICU in Canada
5.1 per 100,000 live births in Germany
Male and female equal
<10% is idiopathic.
22. RISK FACTORS
Indwelling vascular catheter is the single greatest risk factor for
arterial or venous thrombosis.
Indwelling catheters are responsible for >80% of venous and
90% of arterial thrombotic complications.
Others:
Maternal: autoimmune disorder, PROM, IUGR, diabetes, pre-
eclampsia, oligohydramnios, prothrombotic disorder,
chrioamnionitis, family history of thrombosis, antiphospholipid or
anticardiolipin antibody.
Delivery: instrumentation, traumatic delivery, emergency cesarean
section. FHR abnormalities
27. Inherited thrombotic Disorders
Early age of onset,
Spontaneous thrombotic events
Extensive venous thrombosis
Ischemic skin lesions or purpura fulminans
A positive family H/O neonatal purpura fulminans
28. SPECIFIC CLINICAL CONDITIONS ….
Venous thrombosis : Deep vein thrombosis
Difficult to determine
May be clinically silent
Present with swelling and discoloration of limb or face
and head, superior vena cava syndrome
May progress to pulmonary embolism or neonatal stroke
29. Right atrial thrombosis:
Thrombosis of superior vena cava with extension in to
the right atrium
6% of all neonatal thrombosis
>50% asympmtomatic, detected incidentally during
echo
50% present with respiratory distress, new murmur,
heart failure, tachyarrythmia
30. Renal vein thrombosis:
Upto 10% of venous thrombosis in newborn
80% of non catheter related thrombosis.
Common on the left side
Classical triad includes hematuria, palpable abdominal
mass and thrombocytopenia.
Other features- HTN, proteinuria, renal impairment.
USG- enlarge echogenic kidneys with attenuation or loss
of cortico-medullary differentiation.
Color flow doppler- absence of flow in the main or
arcuate renal vein
Complication : adrenal hemorrhage, renal failure, HTN
31. Venous thrombosis: cerebral sinovenous thrombosis
Thrombosis of cerebral veins or dural sinus
Superior and lateral sinuses most frequently involved
Present with seizure, apnea, lethargy
32. Arterial thrombosis: arterial ischemic stroke (AIS)
Mostly occur in middle cerebral artery of left
hemisphere.
AIS is a common underlying cause of neonatal seizures
in full term newborn.
Present with seizures, apnea, asymmetrical motor
development, hemiplagia.
Long term morbidity in 1/3rd
affected newborn are
hemiparesis, speech delay, language delay.
33. Arterial thrombosis: Purpura fulminans
Rare, rapidly progressive, often fatal
Present with DIC and hemorrhagic necrosis of the skin
due to dermal vessel thrombosis.
Due to protein C or S deficiency
34. Approach to thromboembolism
History:
Family history of such disorder
Maternal history of SLE and/or anti-phospholipid syn
Positive risk factor
Treatment history
Physical Examination:
Assessment of severity
Area of involvement
Skin color & compare with other extremity- whether swollen,
cyanotic, hyperemic, discolored, distended superficial vein
Pulses of affected extremity
Presence of any catheter
Assessment of vital organ function.
35. Laboratory studies
1. Coagulation profile: PT, aPTT, TT, plasma fibrinogen
conc.
2. Hct
3. Platelet count: thrombus itself and heparin can cause
thrombocytopenia
4. Genetic test: Protein C and S activity levels
Antithrombin activity assay,Factor V G1691A (Leiden
mutation), Prothrombin G 20210A.
36. Imaging and other study
According to organ involvement:
Real-time USG with color doppler for diagnosis and
monitoring.
Contrast angiography ( the gold standard)
Contrast venography
A plain radiograph of the abdomen for catheter
placement.
USG or CT of head for sinovenous thrombosis or IVH.
MRA for ischemic neonatal stroke
37. “Recommendations for neonatal treatment are
based on -
extrapolation of principles of therapy from
older children & adult guidelines,
limited clinical information from registries,
individual case studies and
knowledge of current common clinical
practice”
38. Management of Neonatal Thrombosis
Supportive care
Anticoagulation
Thrombolysis
Surgery
Counseling
39. Supportive care:
Prompt removal of catheter if possible
Emergency consultation
Local care of the wound
Elevation of foot
Treamtent of
volume depletion
Electrolyte imbalance
Sepsis
Anemia
Thrombocytopenia
40. Choice of therapy
Small asymptomatic non-occlusive arterial or venous
thrombi related to catheters:
Catheter removal and supportive care .
Large or occlusive arterial /venous thrombi :
Anticoagulation with heparin or LMWH
Massive venous thrombi or arterial thrombi:
Thrombolysis
Surgery
[NB- Oral anticoagulant drugs – not recommnaded
for neonate]
41. Anticoagulation
Unfractionated heparin:
Heparin binds with antithrombin III (AT), causing
conformational change that inactivates thrombin and other
proteases most notably factor Xa.
Target aPTT level 60-85 seconds
Duration 5-14 days but can be used upto 3 months.
Reversal agent protamin
Complications : Bleeding, Heparin-induced thrombocytopenia,
osteoporosis
42.
43. Unfractionated Heparin Dosage Monitoring
Dose Check APTT
loading 75 U/Kg After 4 hrs
Maintenance 28 U/Kg/hr Daily or 4 hrs after dose
change
Adjust APTT level as
below:
APTT <50 sec Increase by 20% After 4 hrs
APTT 50-59 sec 10% 4 hrs
APTT 60-85 sec ---------------------- 24 hrs
APTT 86-120 sec Decrease by 10% 4 hrs
APTT >120 Stop for 1 hr then
decrease by 15%
4 hrs
44. LMWH (Enoxaparin)
Has less effect on thrombin compared to heparin, but
about the same effect on Factor Xa.
Duration 5 days to 6 months
side effects : No major bleeds in premature neonates
Soreness from injection/catheter, leakage, bruising .
46. Dosage Monitoring and Adjustment of LMWH
LMW
Heparin(ENOX
APARIN)
Dose 1.5 mg/kg/dose twice daily
Monitoring anti-factor Xa Level (Therapeutic level is 0.5—
1.0 U/ml)
Check 4-6 hrs after first dose( if in therapeutic
range check once weekly)
If dose adjusted recheck after 4 hrs.
If <0.35 units/ml , Increase by 25%
If 0.35-0.49 U/ml , increase by 10%
If 1.1 -2 U/ml, decrease by 20-30%
If >2 U/ml withhold until <0.5 & restart at
40% of original dose.
47. Comparison of UFH and LMWH
Heparin LMWH
1. Requires IV access
2. Short term
anticoagulation
(3 days to 3 weeks)
3. More side effects
4. needs continuous
monitroing
1. Subcutaneous injection
2. Long term
anticoagulation
( upto 6 months)
3. Fewer side effects
4. Needs less monitoring
48. Goal-
to degrade fibrin
dissolve fibrin clot
Indication: Not recommended unless major vessel
occlusion causing critical organ or limb compromise.
Outcome: In older children vascular patency 50%
with anticoagulant therapy, following thrombolytic
therapy > 90%.
If thrombolytic treatment >24 hours monitor
plasminogen conc or FFP infusion.
Treatment with heparin after thrombolytic therapy is
recommended.
Thrombolytic Therapy
49. Thrombolytic Agents
tPA :
No loading dose
0.1-0.6 mg/kg/h over 6 h
followed by heparin
Streptokinase:
Loading-2,000 U/kg over 10 min then
1,000-2,000 U/kg/h .Only one course should be given
for 6 h
Urokinase:
52. Surgical thrombectomy
Not done in majority of neonates
Microsurgery with thrombolytic regimen is
successfully used in few isolated cases.
53. Precautions
Intramuscular (IM) injections and arterial punctures
during anticoagulation or thrombolytic therapy should be
avoided.
Indomethacin or other antiplatelet drugs during therapy
should be avoided. .
Use minimal physical manipulation of the patient.
Thrombolytic therapy should not be initiated in the presence
of active bleeding.
54. Monitor for thromboembolic complication in all newborn
with any catheter.
heparin is often added to neonatal infusions as it
prolongs patency
Umbilical lines should be removed as early as possible.
UAC <5 days and UVC < 14 days
Prefer a peripheral arterial lines
If there is difficulty infusing consider thrombotic event
Use UAC with a hole at the end not at the side
A PICC lines has lower incidence of thrombosis.