Download as PDF, PPTX


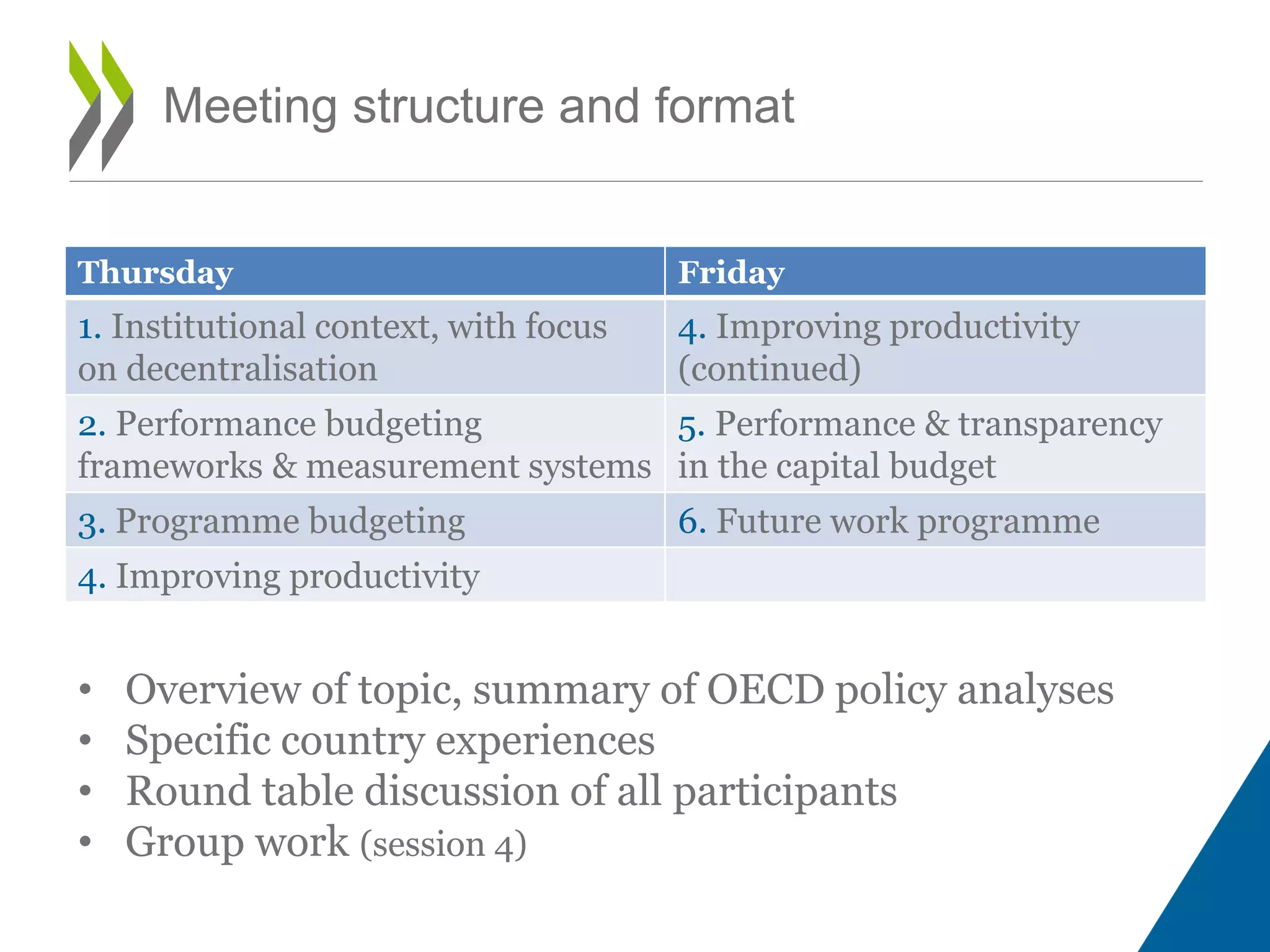

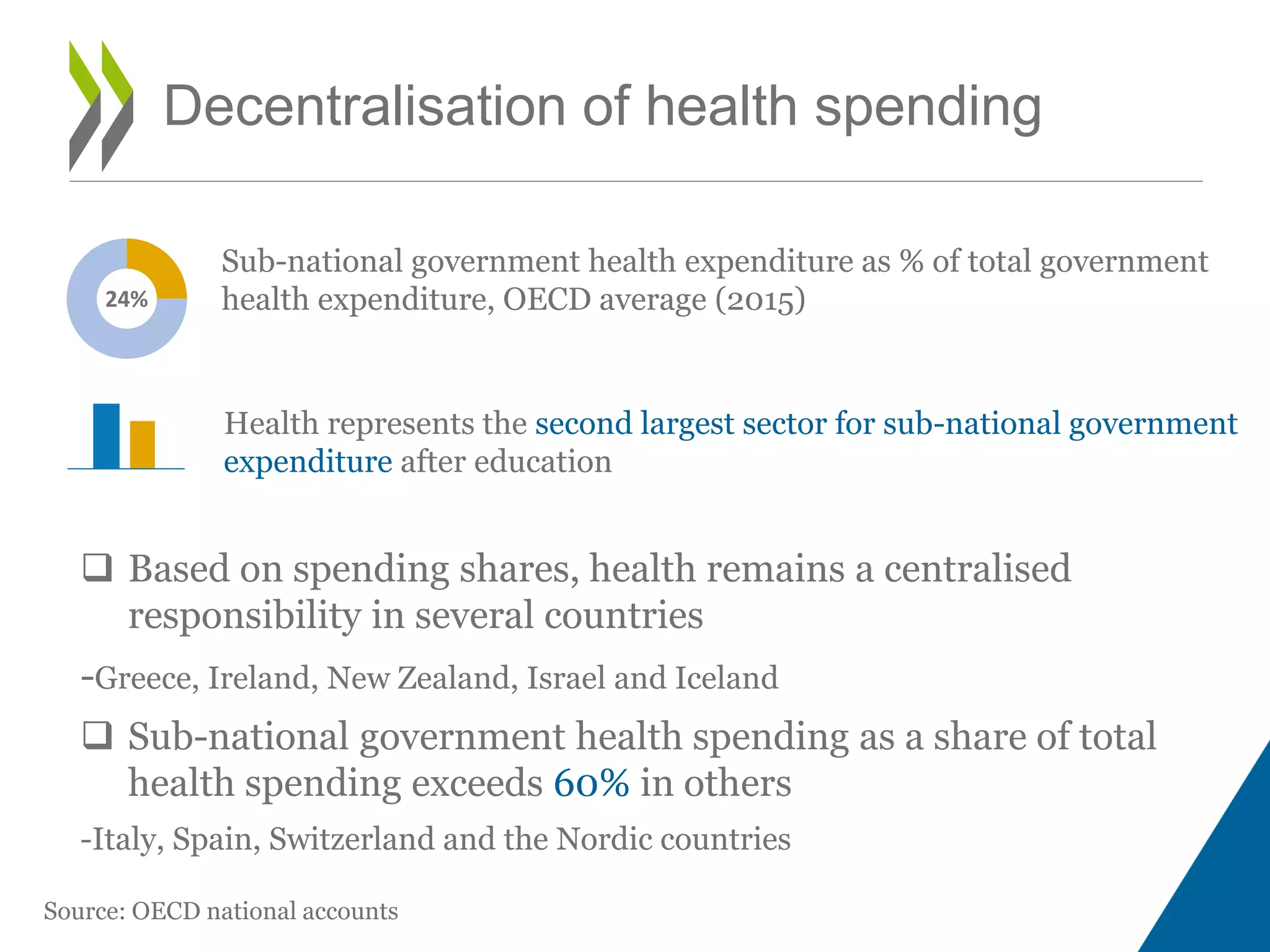
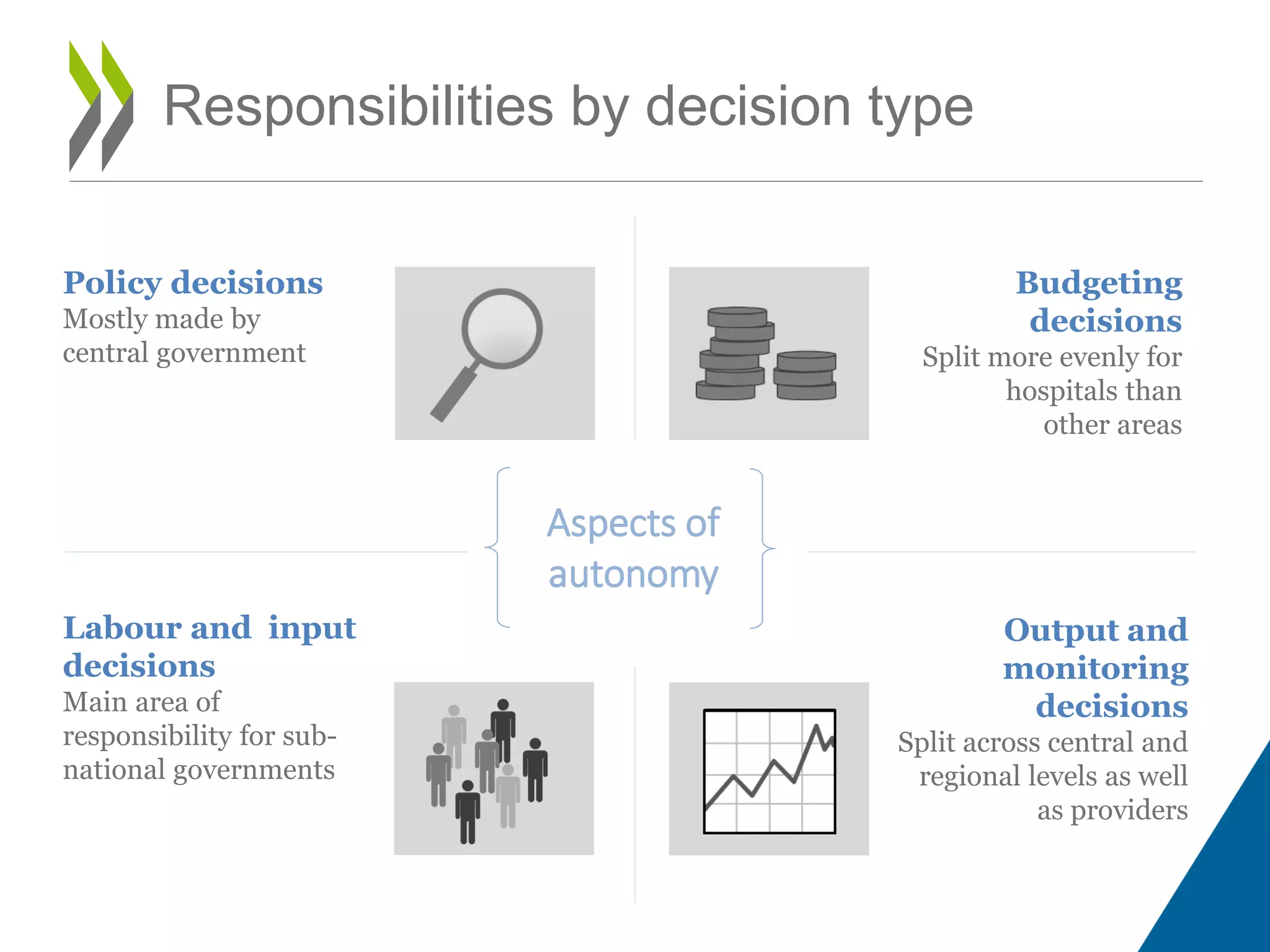

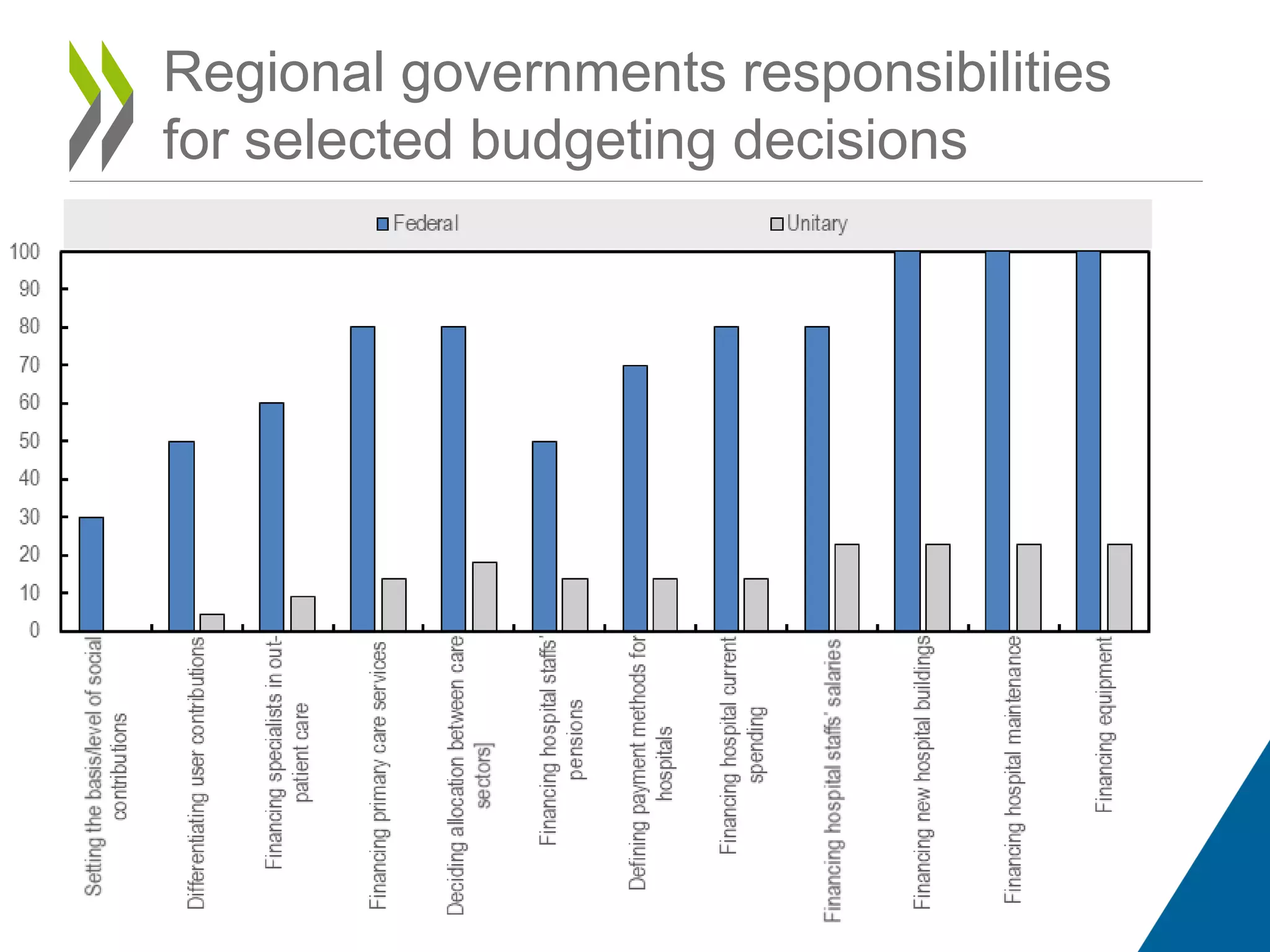
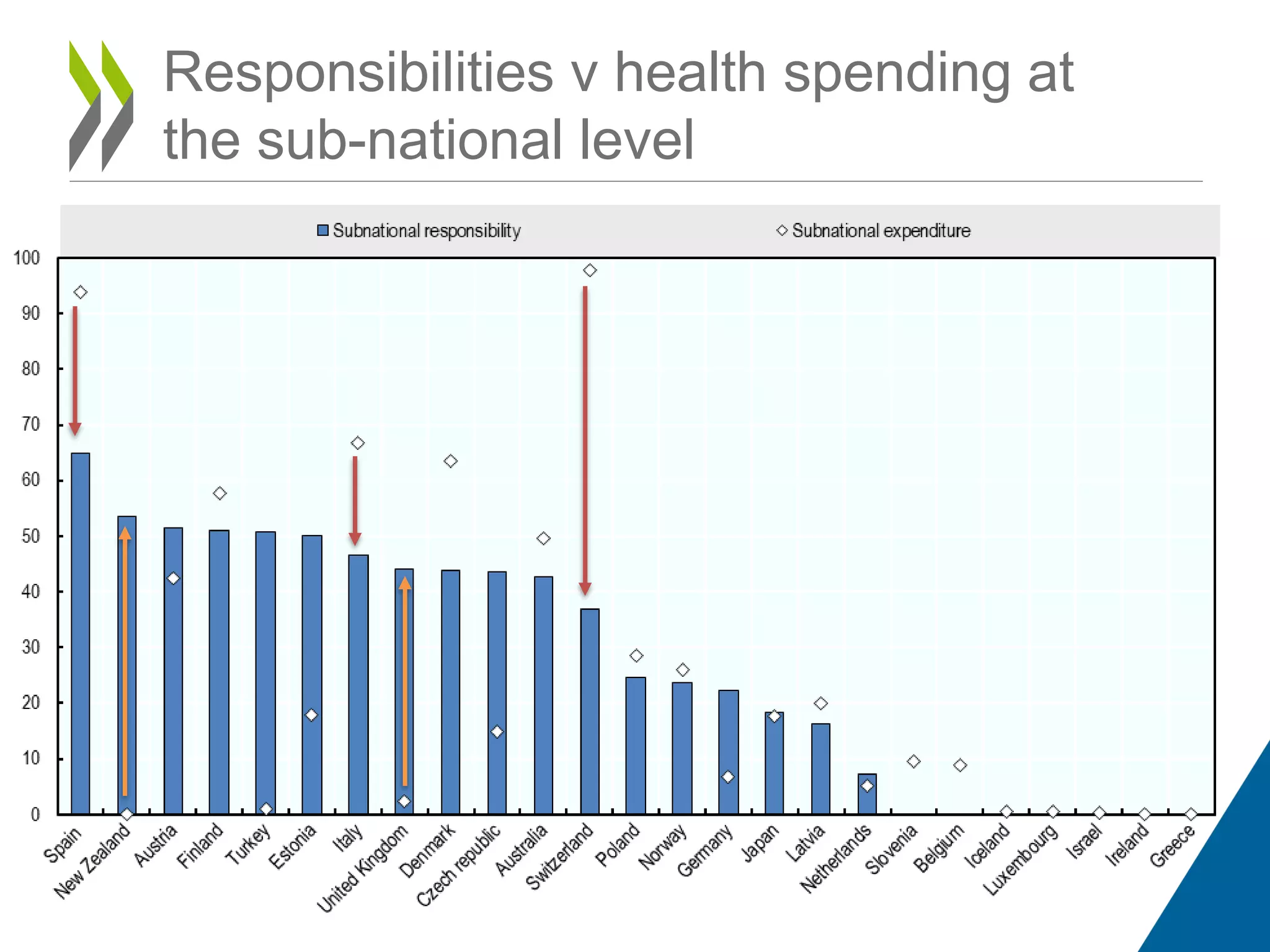

The document outlines a meeting focused on the impact of decentralization on budgetary decisions in health care, emphasizing the need to align health budgets with policy priorities and improve accountability. It discusses the varying degrees of decentralization among OECD countries and highlights the importance of performance budgeting frameworks and measurement systems. The meeting structure includes presentations, discussions, and group work to foster peer-to-peer learning and gather insights from diverse participants.



















































































