Download to read offline



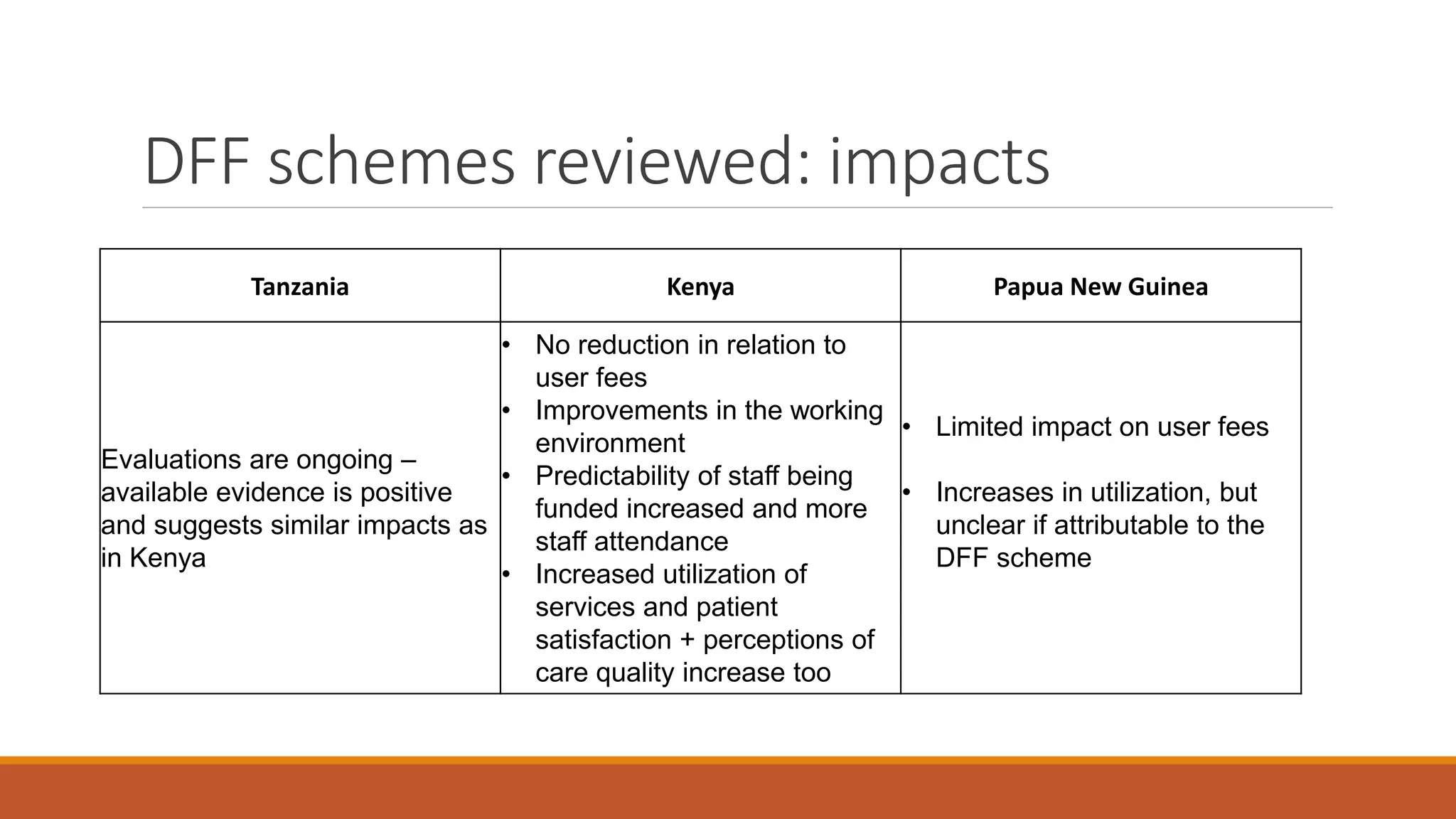
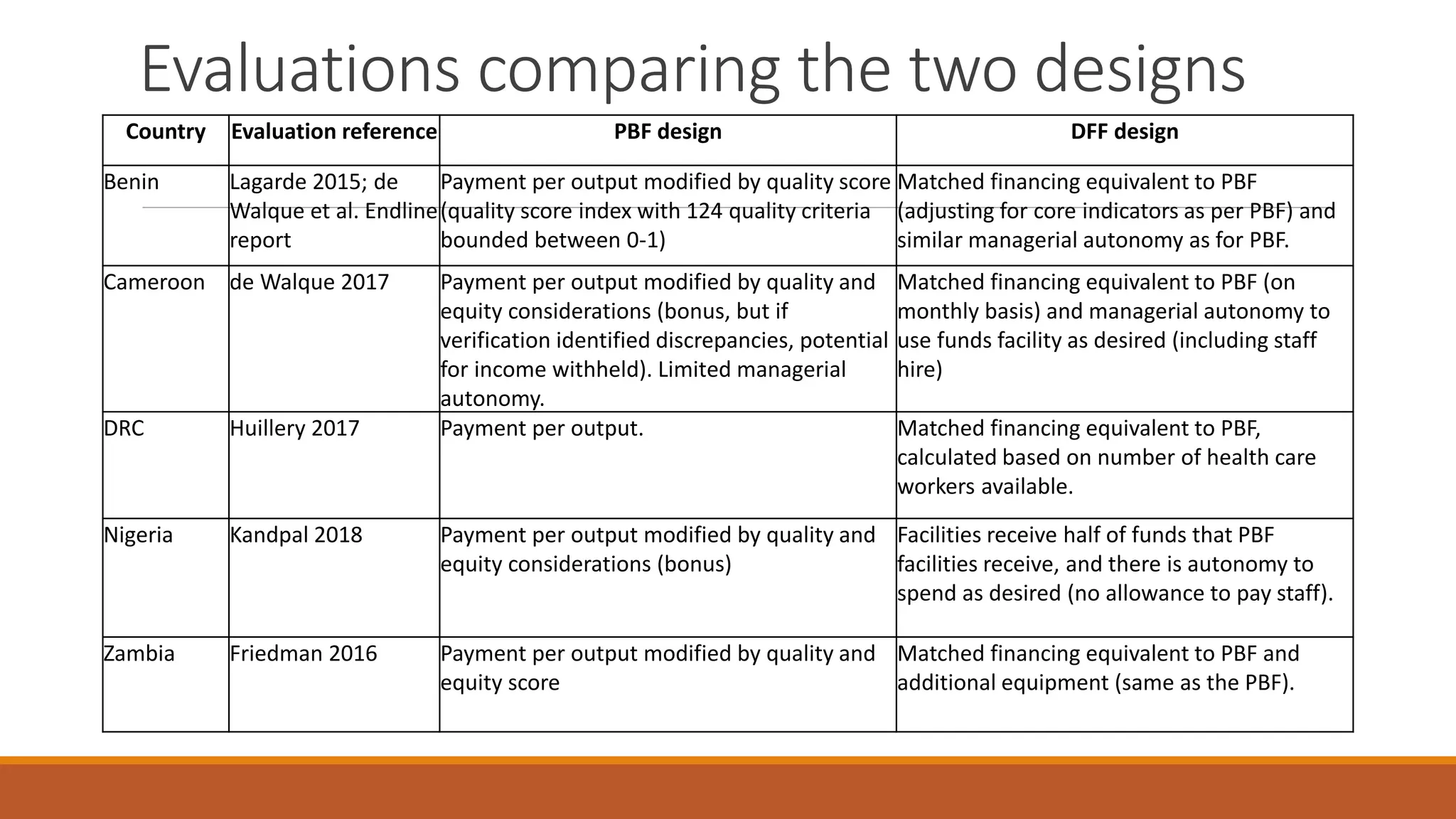
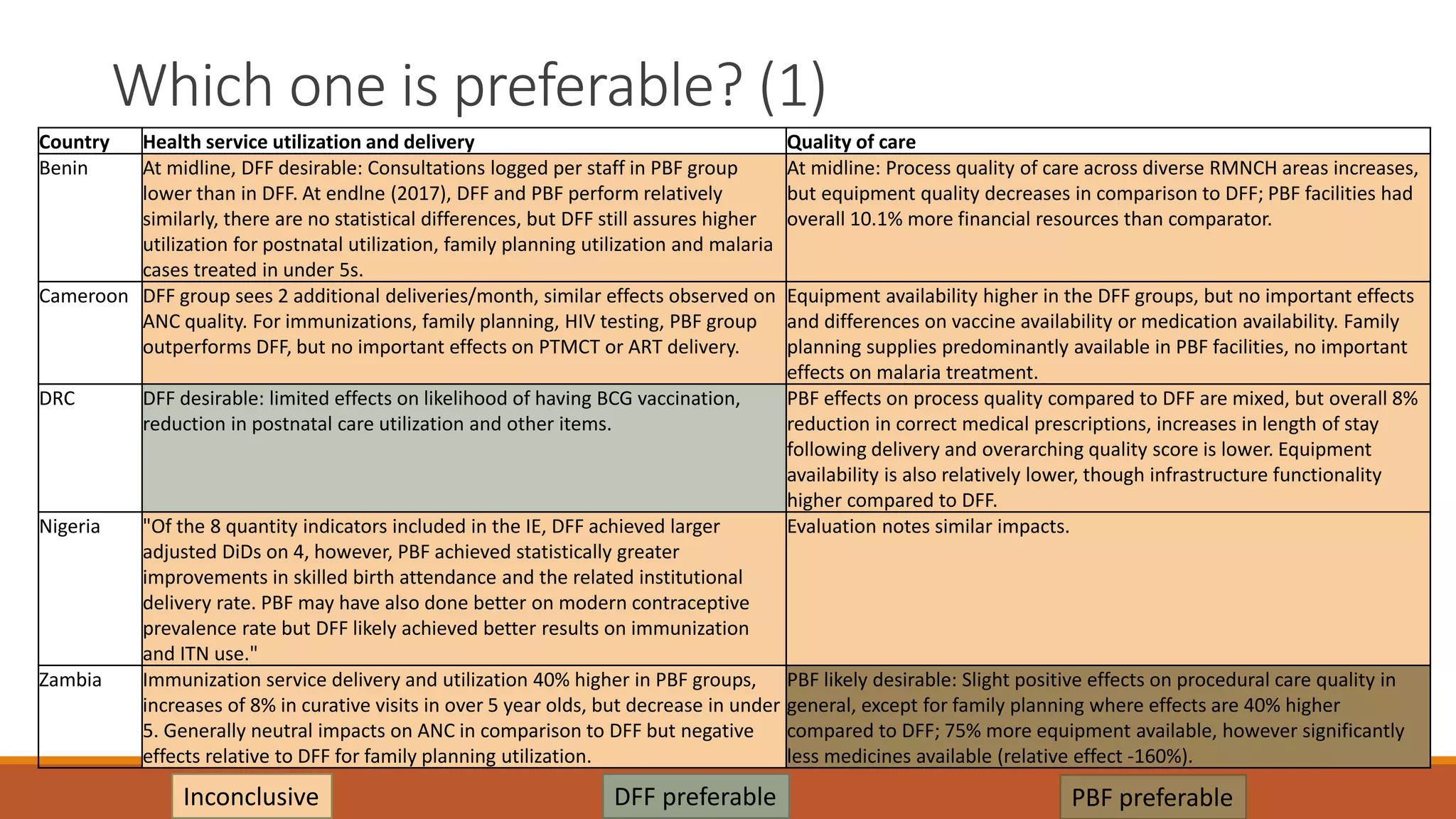


1) The document reviews evidence on the effectiveness of performance-based financing (PBF) and direct facility financing (DFF) approaches. 2) The Cochrane review found that PBF generally improved utilization and quality of targeted health services, but results were mixed for non-targeted indicators. Impacts on health outcomes were also mixed. 3) Evidence on DFF was limited but other reviews found prospective payment mechanisms like capitation can reduce costs while maintaining service utilization and quality of care.












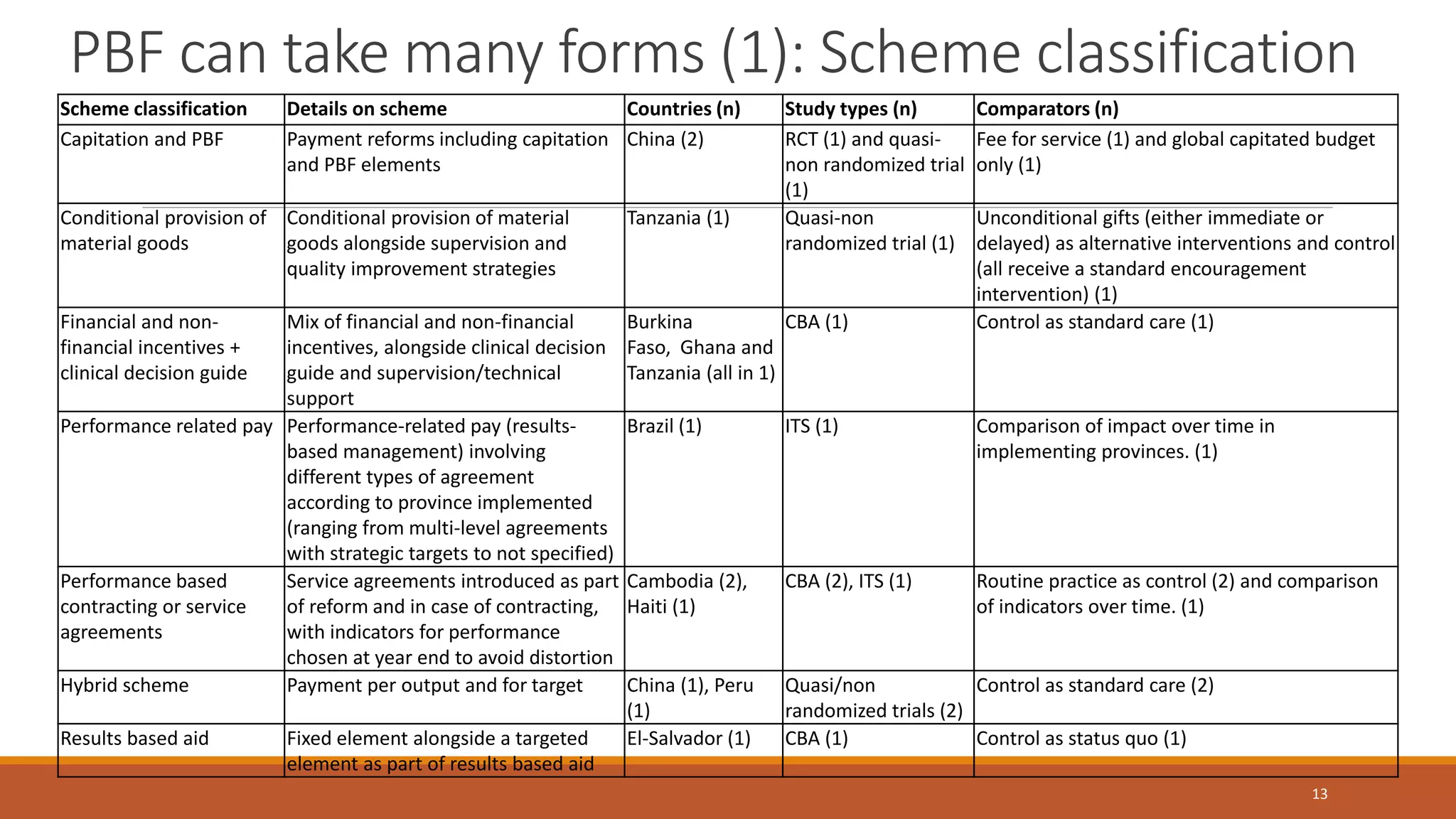
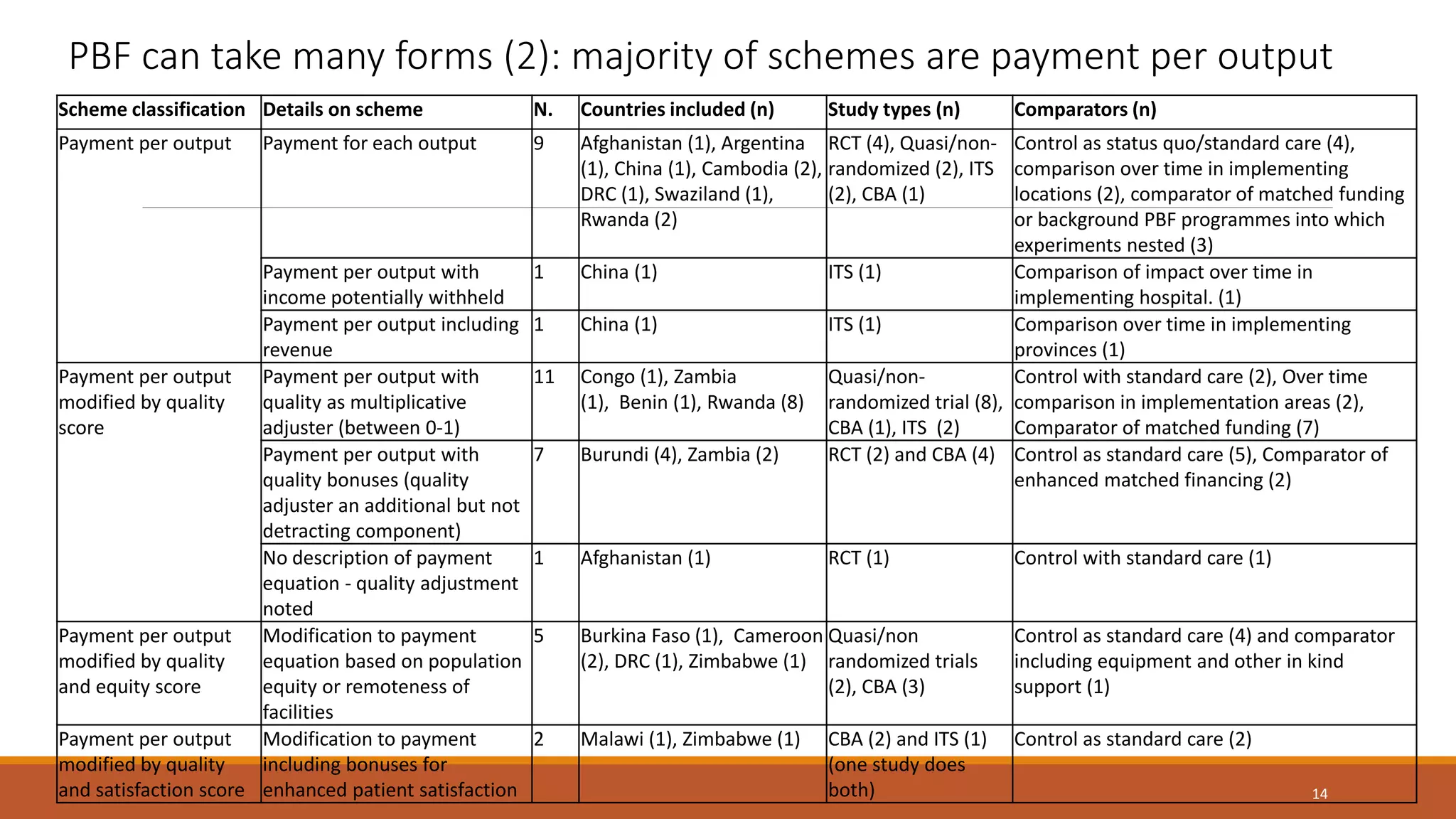
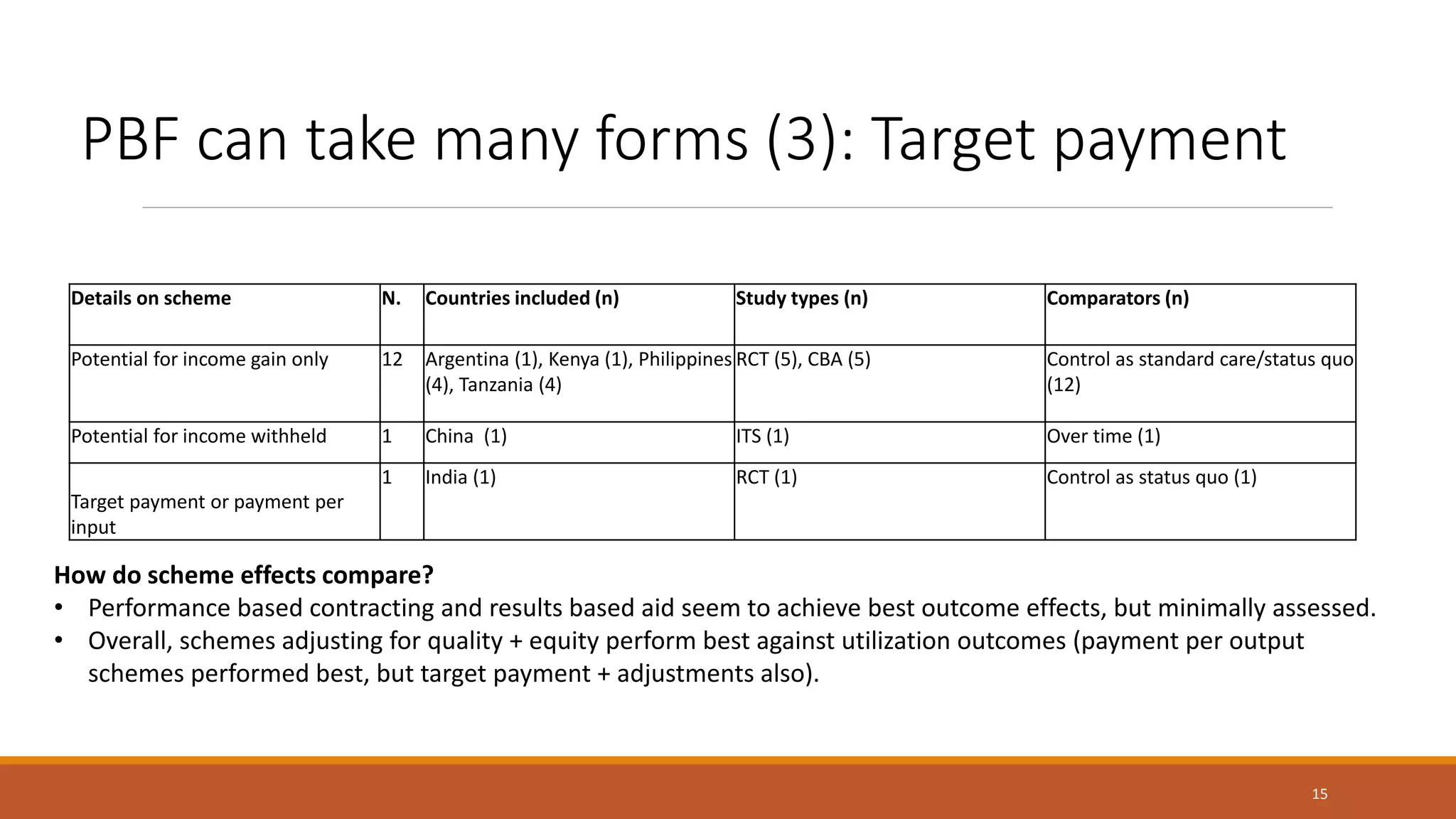
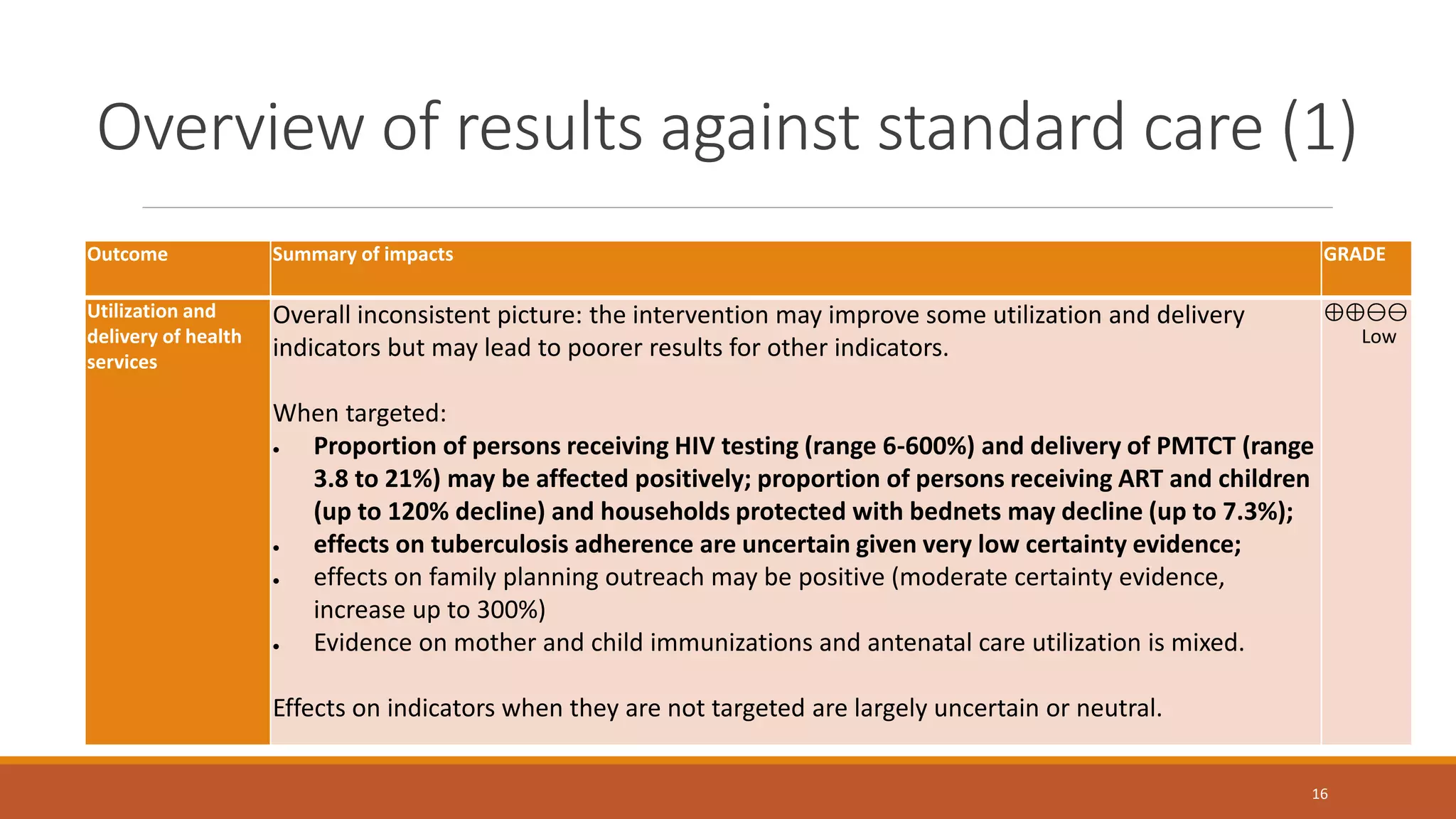
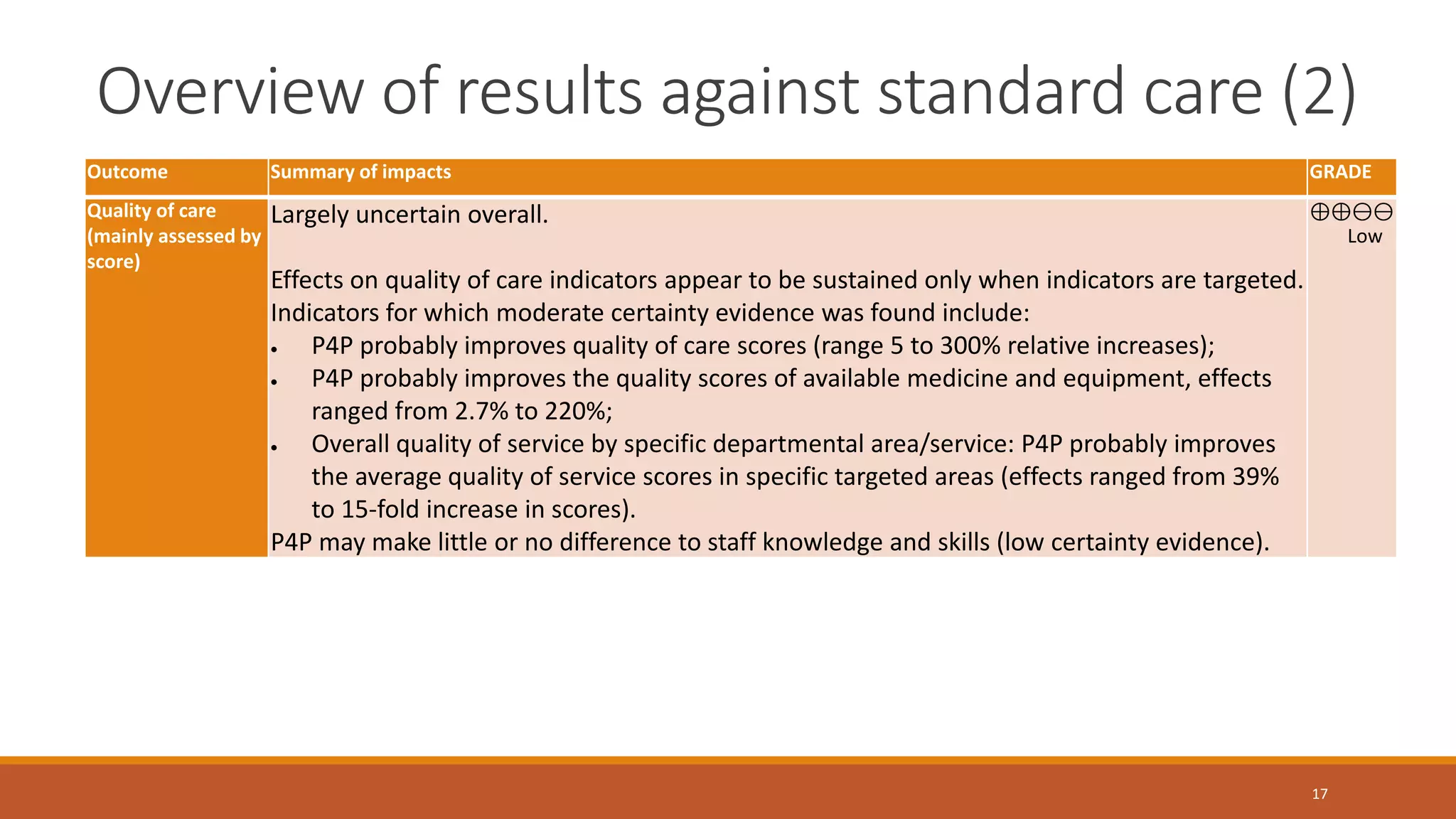
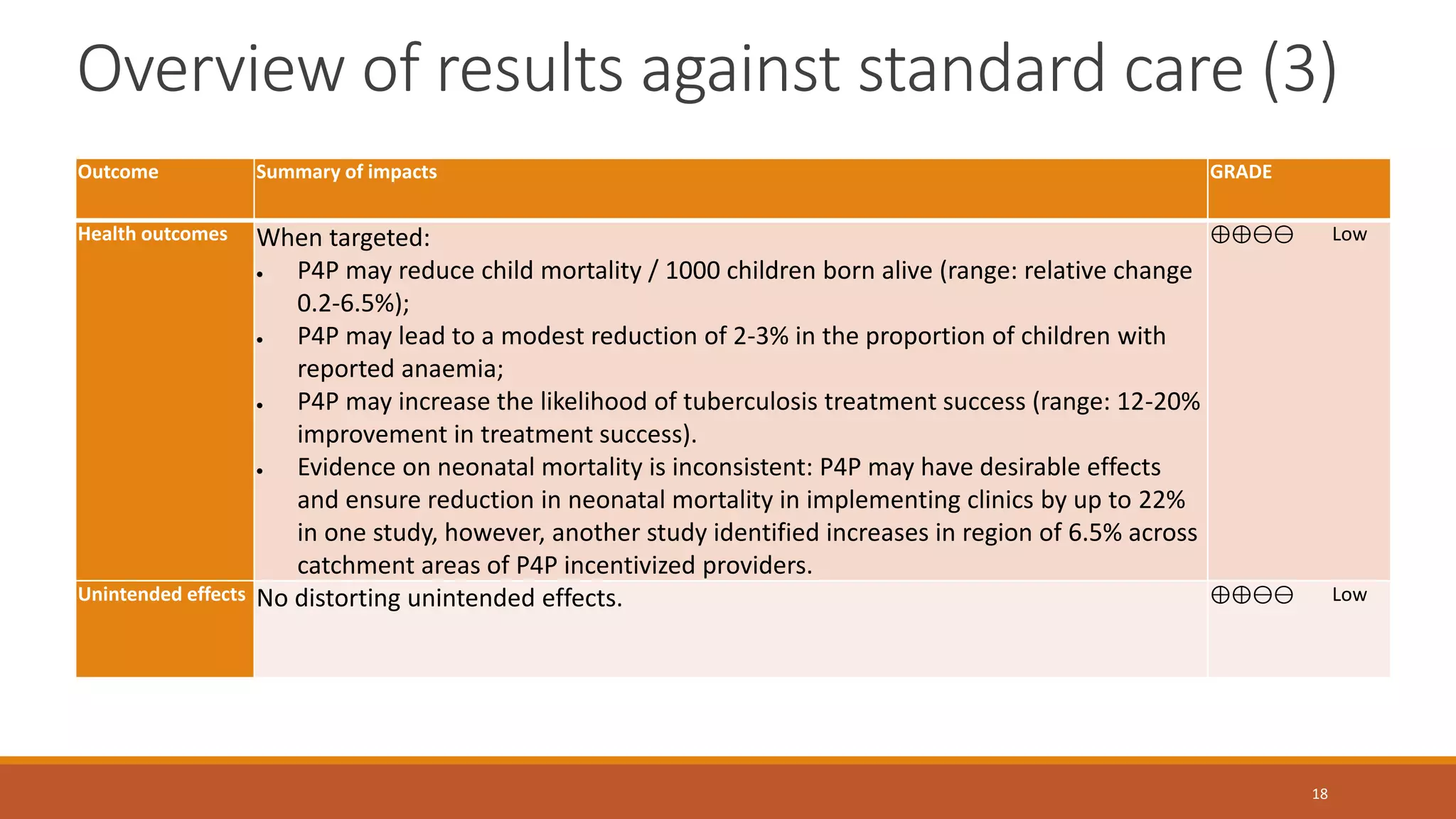
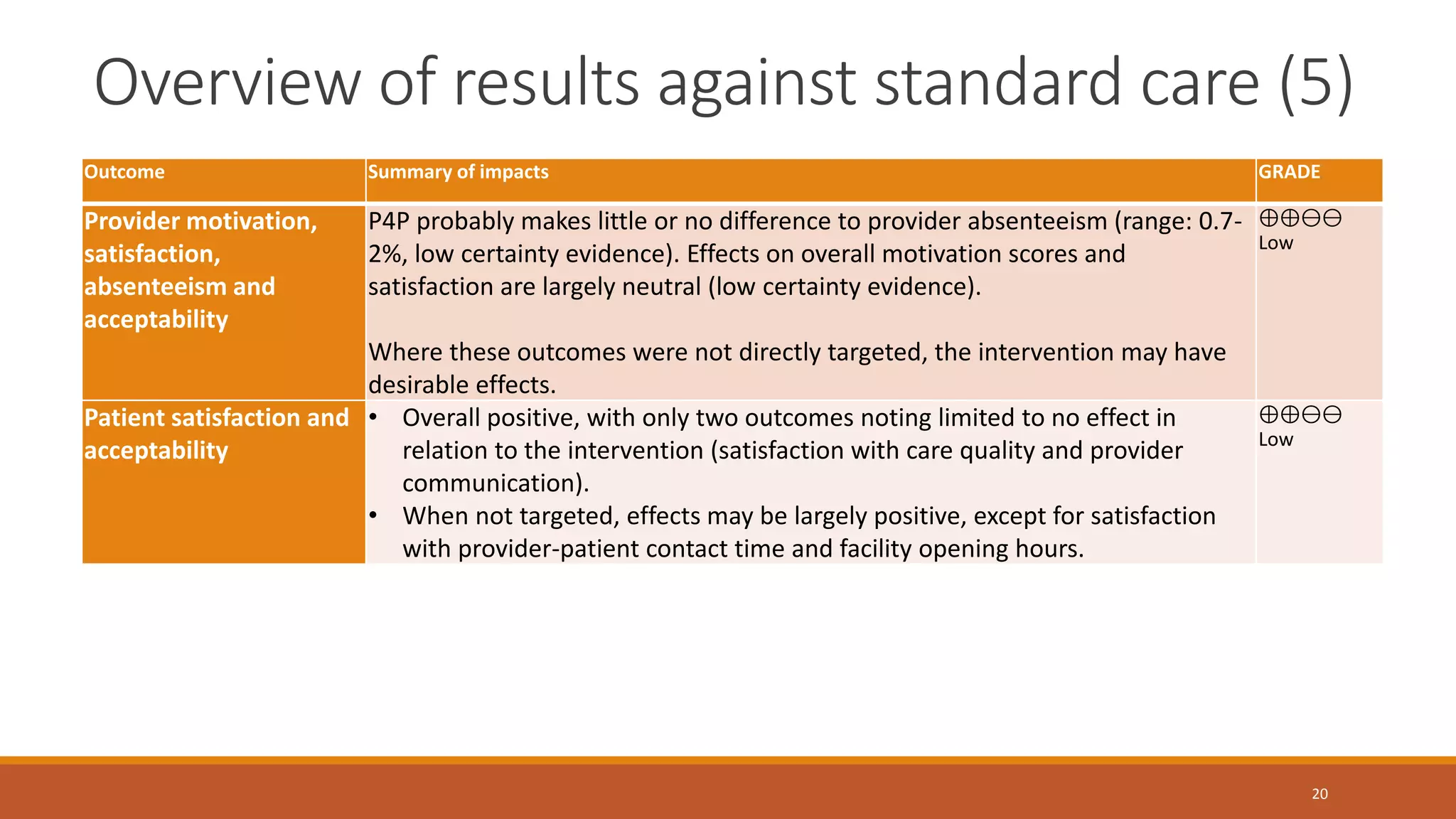
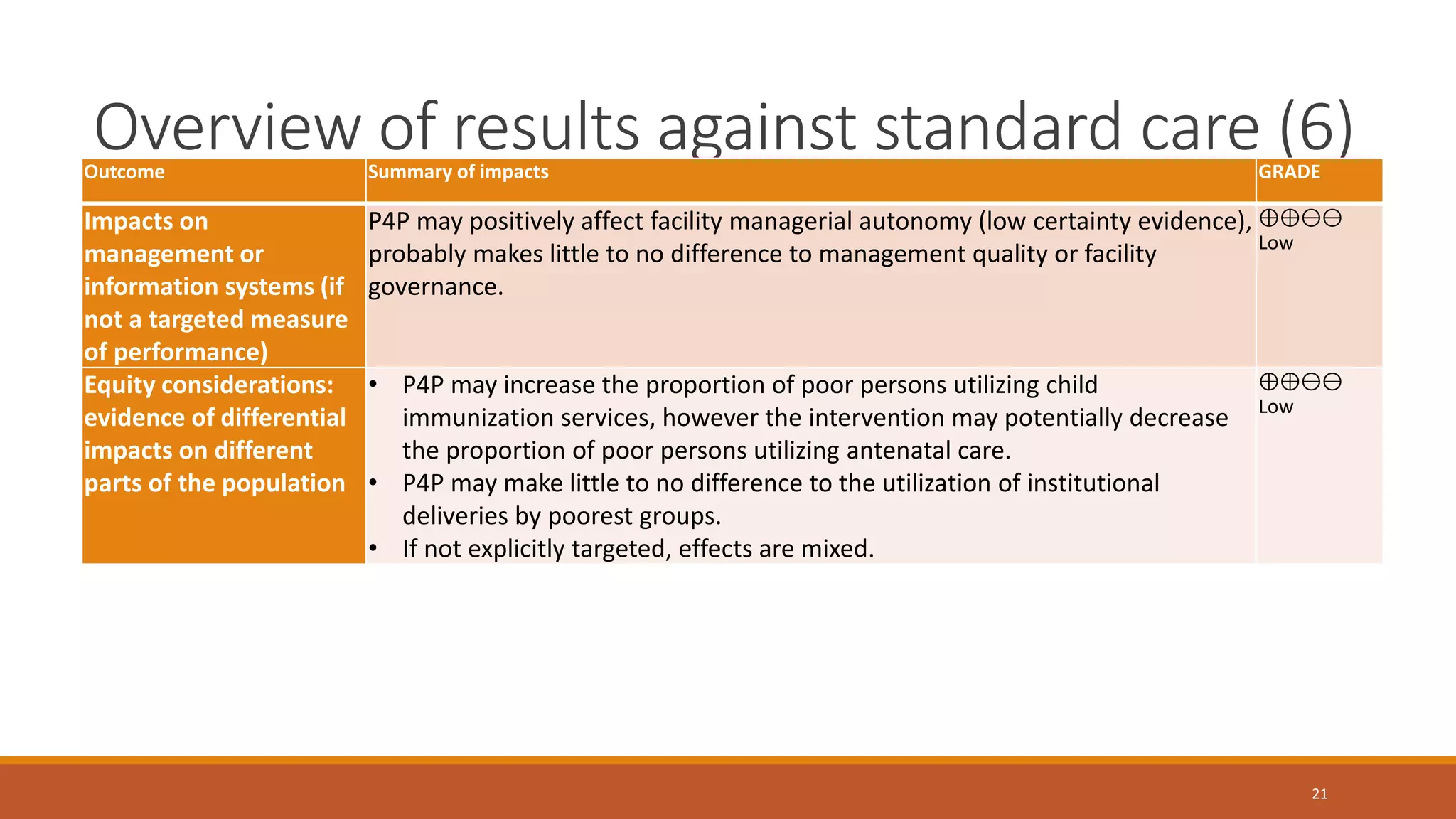
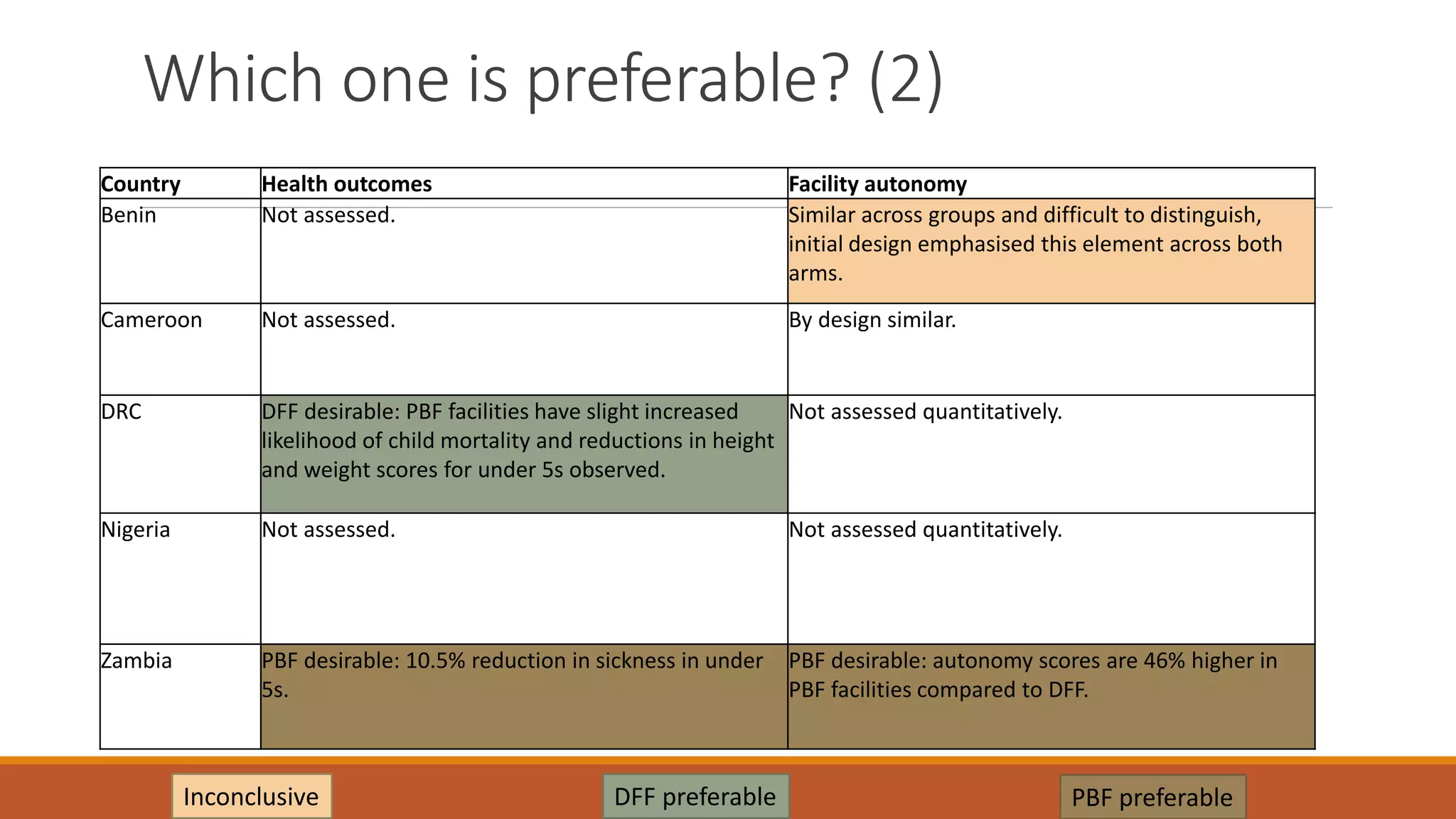
![Trudel Cms Rules 072810[1]](https://cdn.slidesharecdn.com/ss_thumbnails/trudelcmsrules0728101-12814484645456-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)






































































