Download as PDF, PPTX


![Integration and Integrated Care
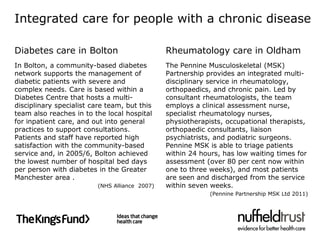
Integration is the combination of processes, methods and
tools that facilitate integrated care.
Integrated care results when the culmination of these
processes directly benefits communities, patients or service
users – it is by definition ‘patient-centred’ and ‘population-
oriented’
Integrated care may be judged successful if it contributes to
better care experiences; improved care outcomes;
delivered more cost effectively
‘Without integration at various levels [of health systems], all aspects of
health care performance can suffer. Patients get lost, needed services fail
to be delivered, or are delayed, quality and patient satisfaction decline,
and the potential for cost-effectiveness diminishes.’
(Kodner and Spreeuwenbur, 2002, p2)](https://image.slidesharecdn.com/evidence-base-integrated-care-111020165301-phpapp01/85/The-Evidence-Base-for-Integrated-Care-6-320.jpg)


















![Resource Pack (3)
NHS Wales (no date) Chronic conditions management demonstrators [on-line]. Available
at: http://www.ccmdemonstrators.com/
The Nuffield Trust (2011) Predictive risk and health care: an overview. London: The
Nuffield Trust. Available at:
http://www.nuffieldtrust.org.uk/sites/files/nuffield/publication/Predictive-risk-and-
health-care-an-overview_0.pdf
Rosen R, et al (2011) Integration in action: four international case studies. London: The
Nuffield Trust. Available at: http://www.nuffieldtrust.org.uk/publications/integration-
action-four-international-case-studies
Shaw S et al (2011) What is integrated care? London: The Nuffield Trust. Available at:
http://www.nuffieldtrust.org.uk/publications/what-integrated-care
Thistlethwaite P (2011) Integrating health and social care in Torbay. Improving care for
Mrs Smith. London: The King’s Fund. Available at:
http://www.kingsfund.org.uk/publications/integrating_health_1.html
Windle K et al (2010) National Evaluation of Partnerships for Older People Projects. Final
Report. Kent: PSSRU. Available at:
http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/docum
ents/digitalasset/dh_111353.pdf](https://image.slidesharecdn.com/evidence-base-integrated-care-111020165301-phpapp01/85/The-Evidence-Base-for-Integrated-Care-56-320.jpg)

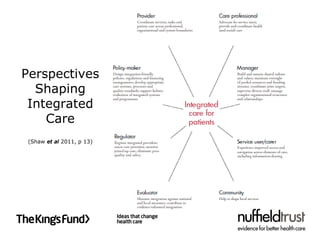
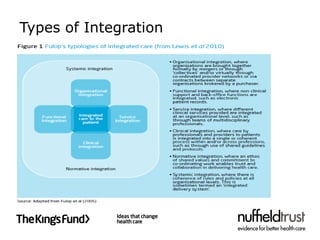
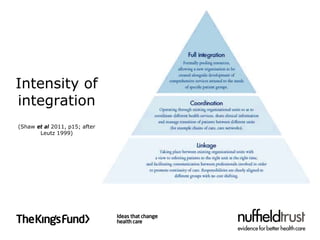
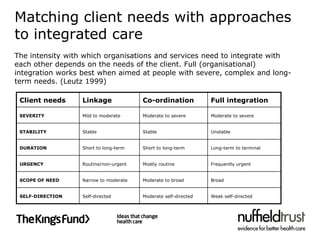
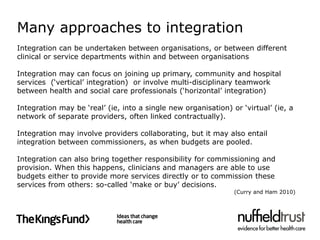
The document discusses integrated care, defining it as an approach to improve health service delivery by addressing fragmentation and ensuring patient-centered care. It highlights the challenges faced in implementing integrated care across different health sectors, including competition, choice policies, and systemic barriers, while providing examples of successful integrated care models in the UK. Key recommendations for promoting integrated care include using various implementation tools, targeting populations in need, and aligning system incentives to facilitate better collaboration among healthcare providers.




































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











