Download to read offline

















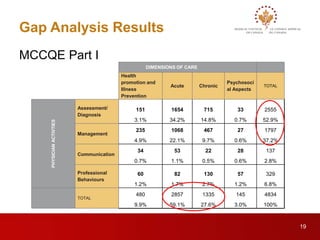




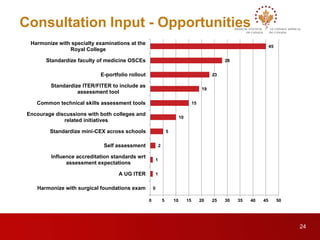








This document outlines the progress of the Blueprint Project since 2013. It proposes common frameworks to assess physicians for high-stakes decision making at two points: entry into residency and independent practice. Stakeholder consultations provided feedback on proposed assessment dimensions and definitions. Gap analyses found MCC exams currently underrepresent chronic illness and psychosocial aspects. Future work includes developing additional assessments through opportunities like e-portfolios and item banks to fully address the blueprint. Workshops will discuss including various assessments in an e-portfolio and sharing assessment data between organizations. The project aims to ensure physicians are qualified for practice through a rigorous yet evolving assessment system.

































































