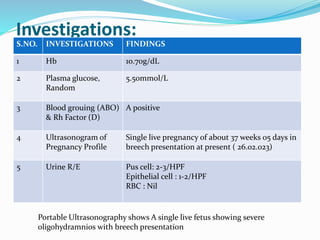
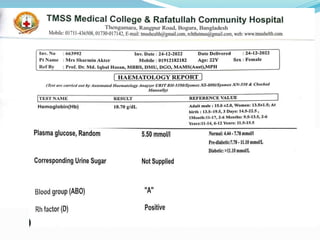
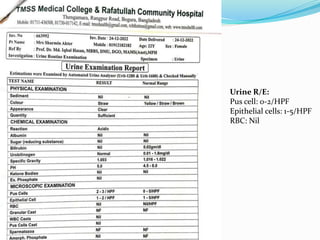
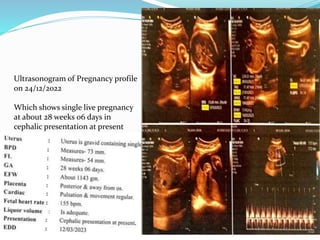
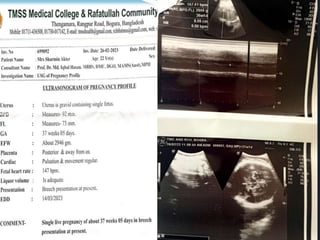
Mrs. Sharmin Aktar, a 28-year-old primigravida, presented with a 38-week pregnancy, experiencing a sudden gush of colorless, odorless vaginal discharge. Clinical examination confirmed a breech presentation with severe oligohydramnios, and she was admitted for management, receiving supportive care and necessary interventions. A lower uterine cesarean section was performed, resulting in the delivery of a healthy male baby weighing 3.2 kg.