Downloaded 40 times
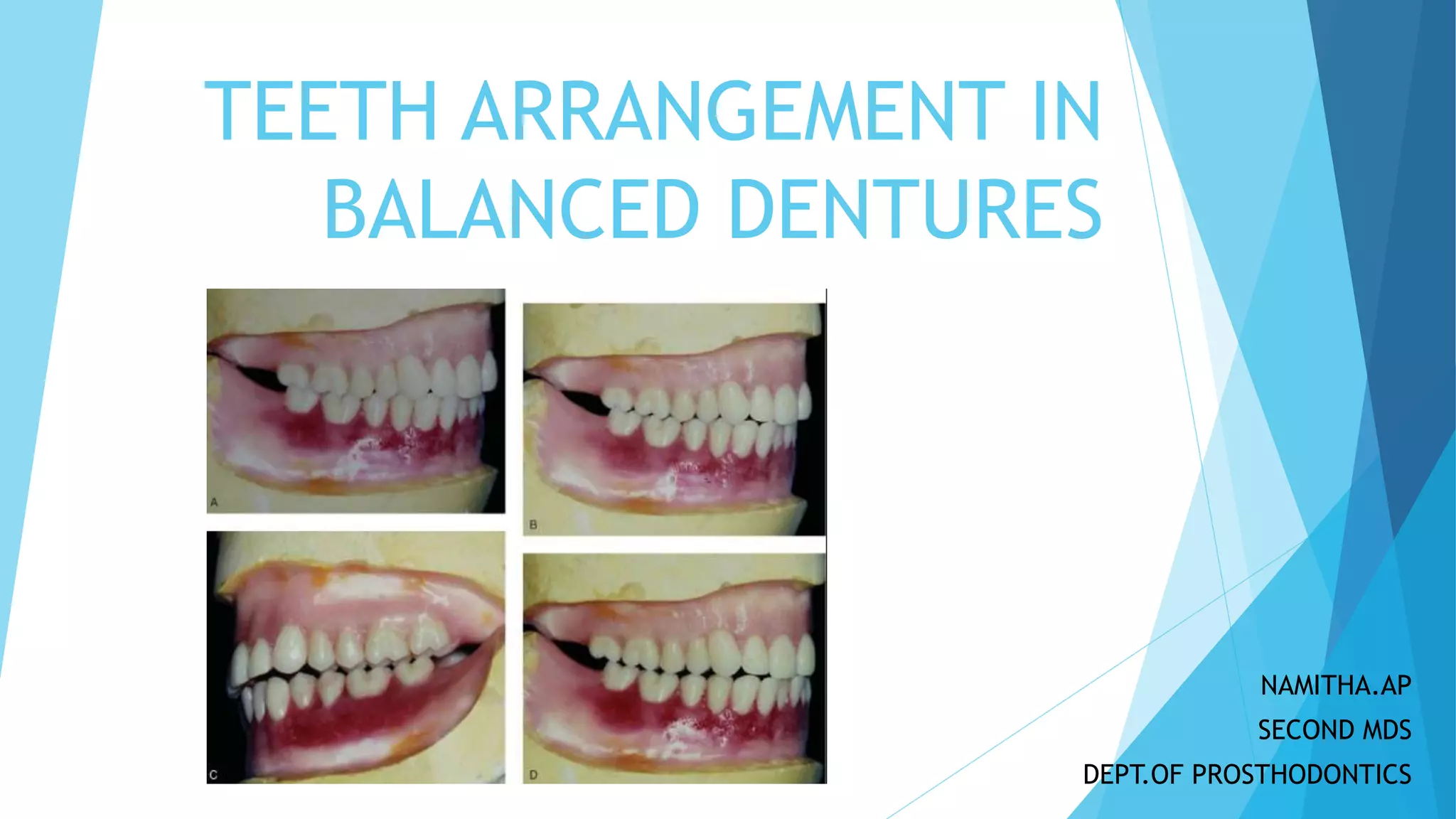



















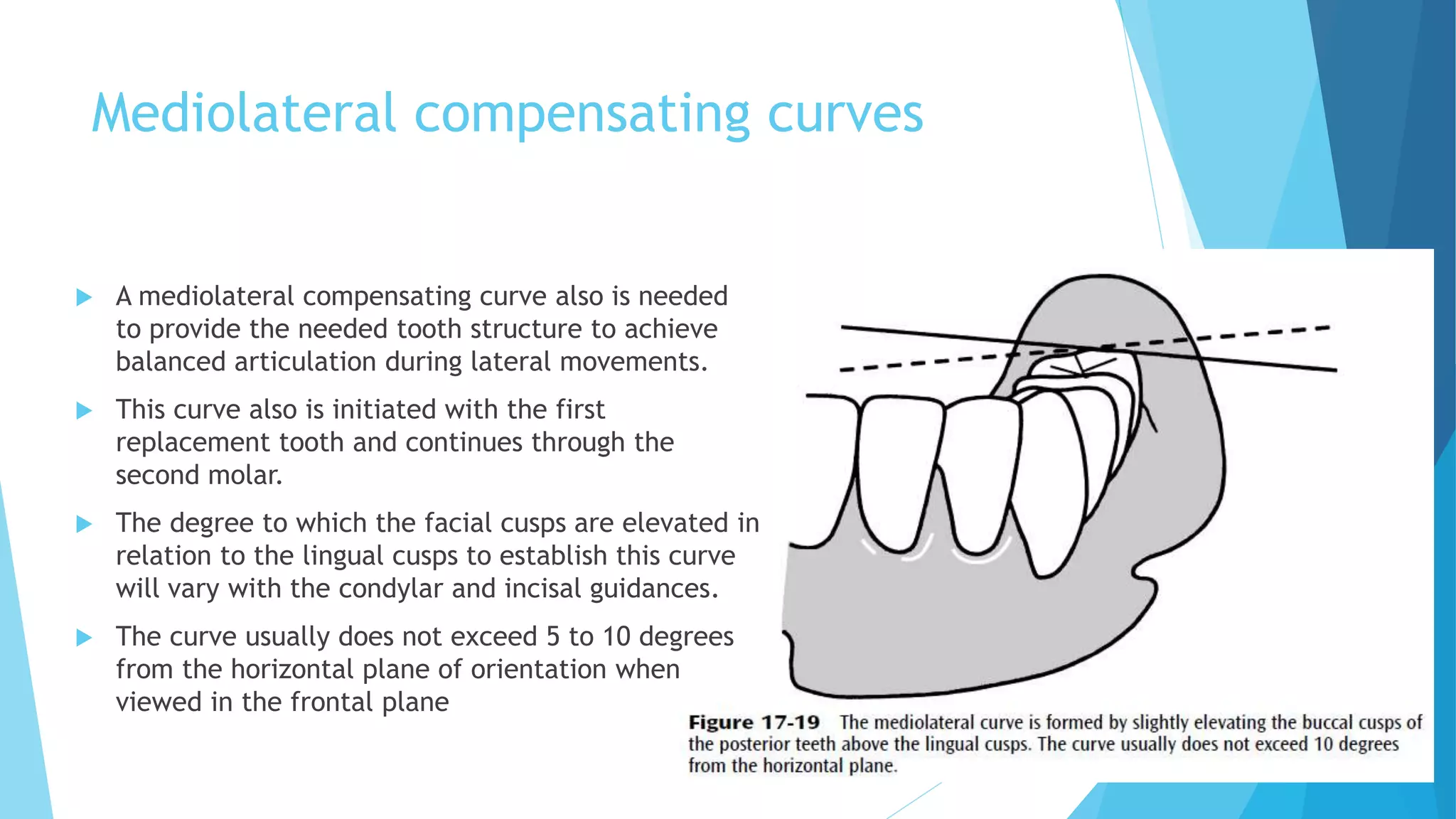







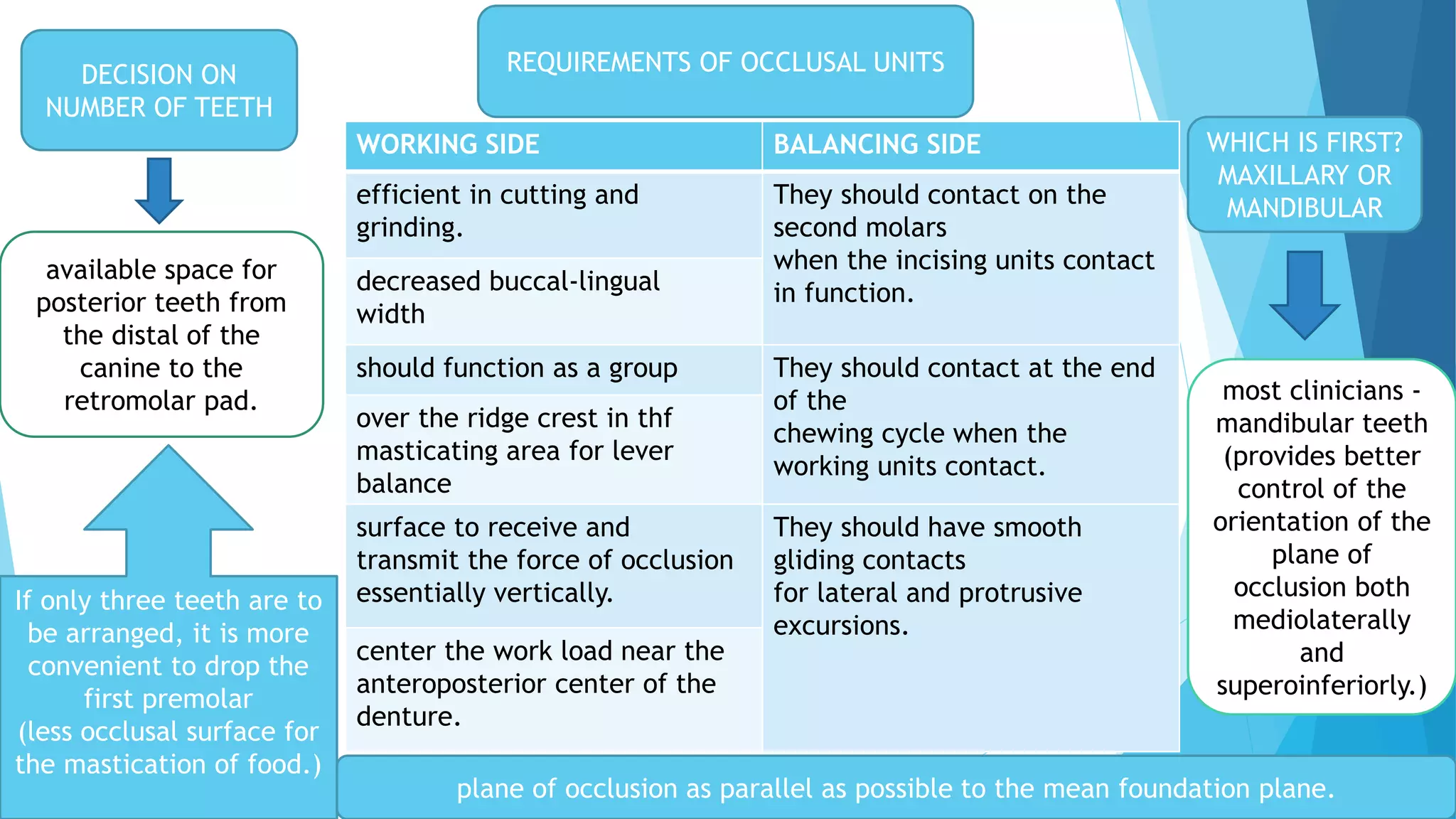
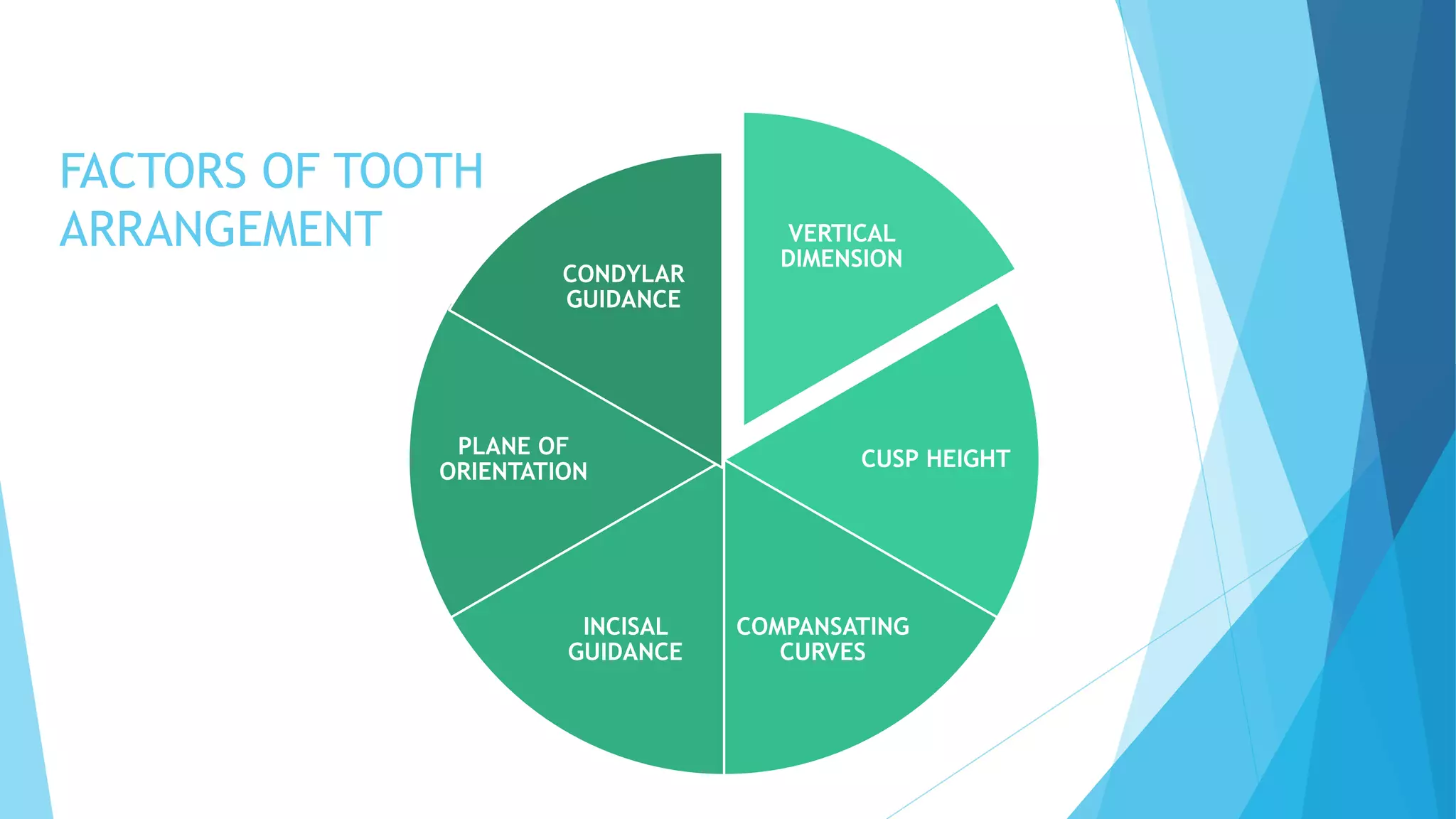




















The document provides detailed guidelines for the arrangement and placement of teeth in balanced dentures, emphasizing alignment with facial features and anatomical considerations. Key factors include the positioning of maxillary and mandibular teeth to ensure aesthetic harmony and proper occlusion, as well as specific instructions for various types of teeth. It also discusses the importance of compensating curves in achieving balanced articulation during movements.























































































