Downloaded 38 times

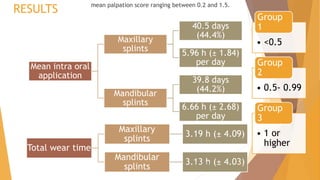
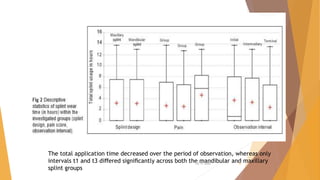









This document summarizes a study that used intraoral sensors to objectively monitor patient compliance with stabilization splint therapy for myofascial pain. Some key findings: - 32 patients were randomly assigned maxillary or mandibular splints equipped with sensors recording wear time. - Overall compliance was 44.4% for maxillary and 44.2% for mandibular splints, with no significant difference between the groups. - Patients with greater pain wore their splints significantly more. Wear time decreased over the 3 observation periods as pain reduced with treatment success. - The study demonstrated intraoral sensors are an effective way to objectively monitor splint wear compared to subjective reports.






















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)