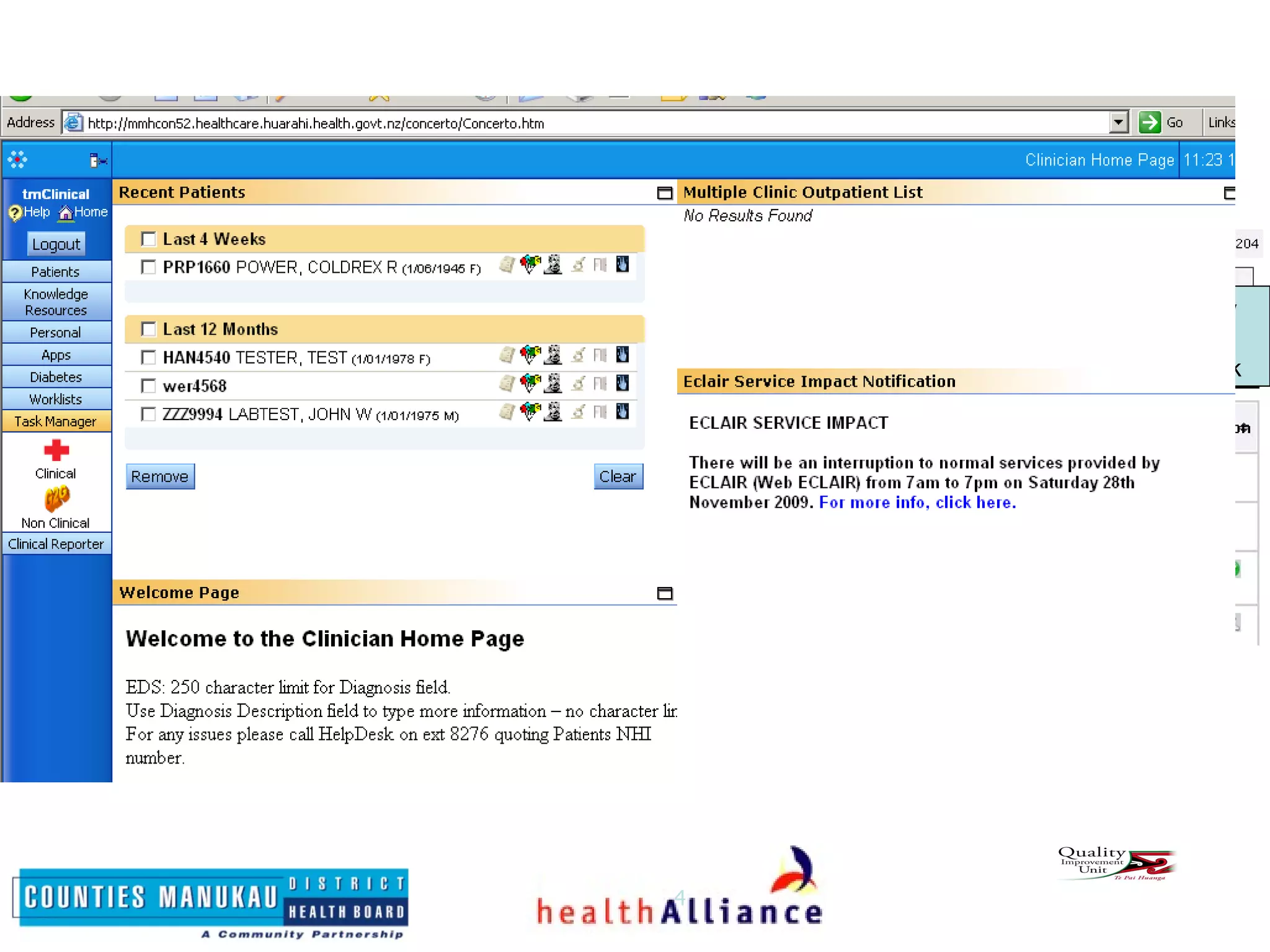
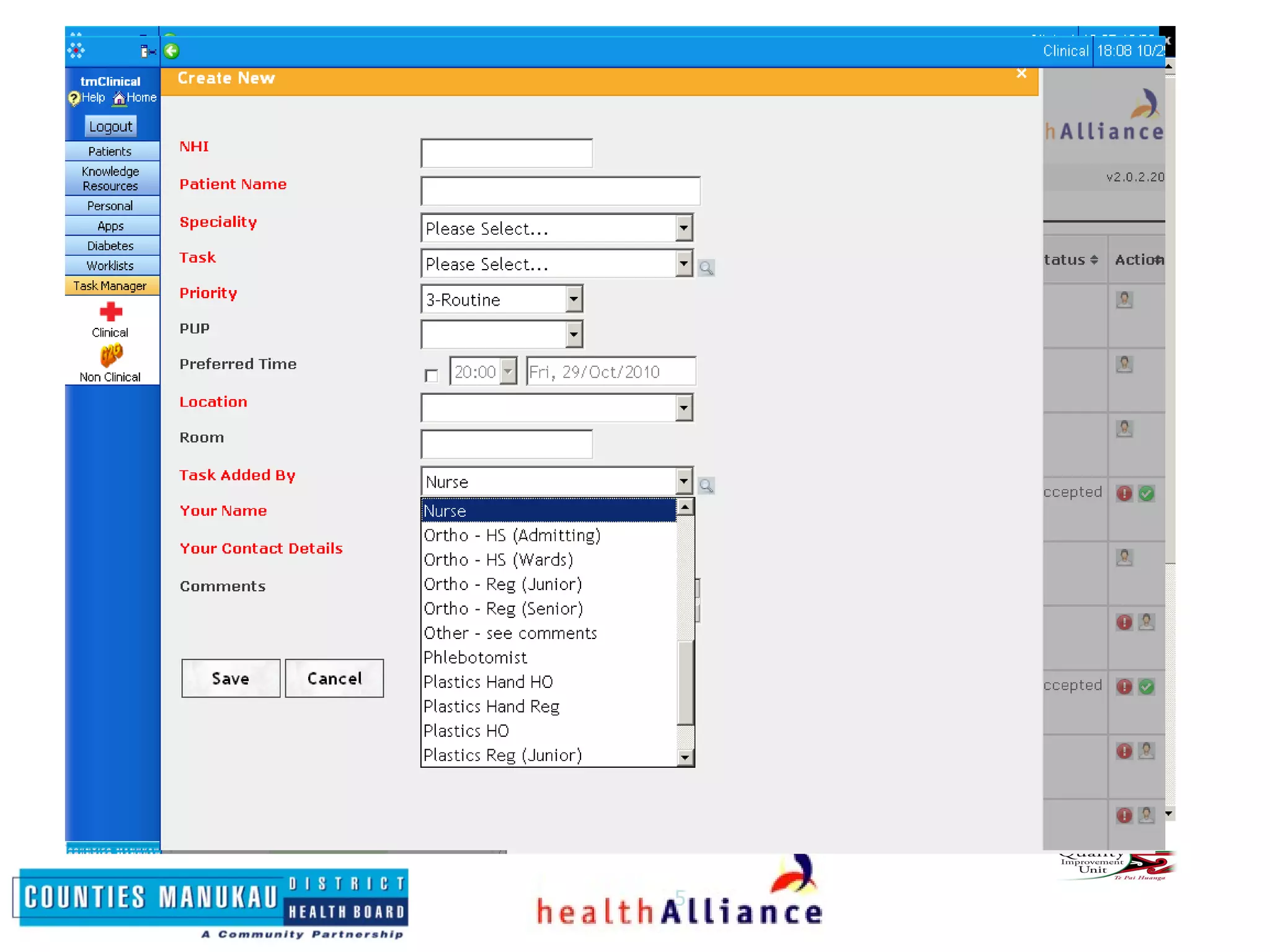
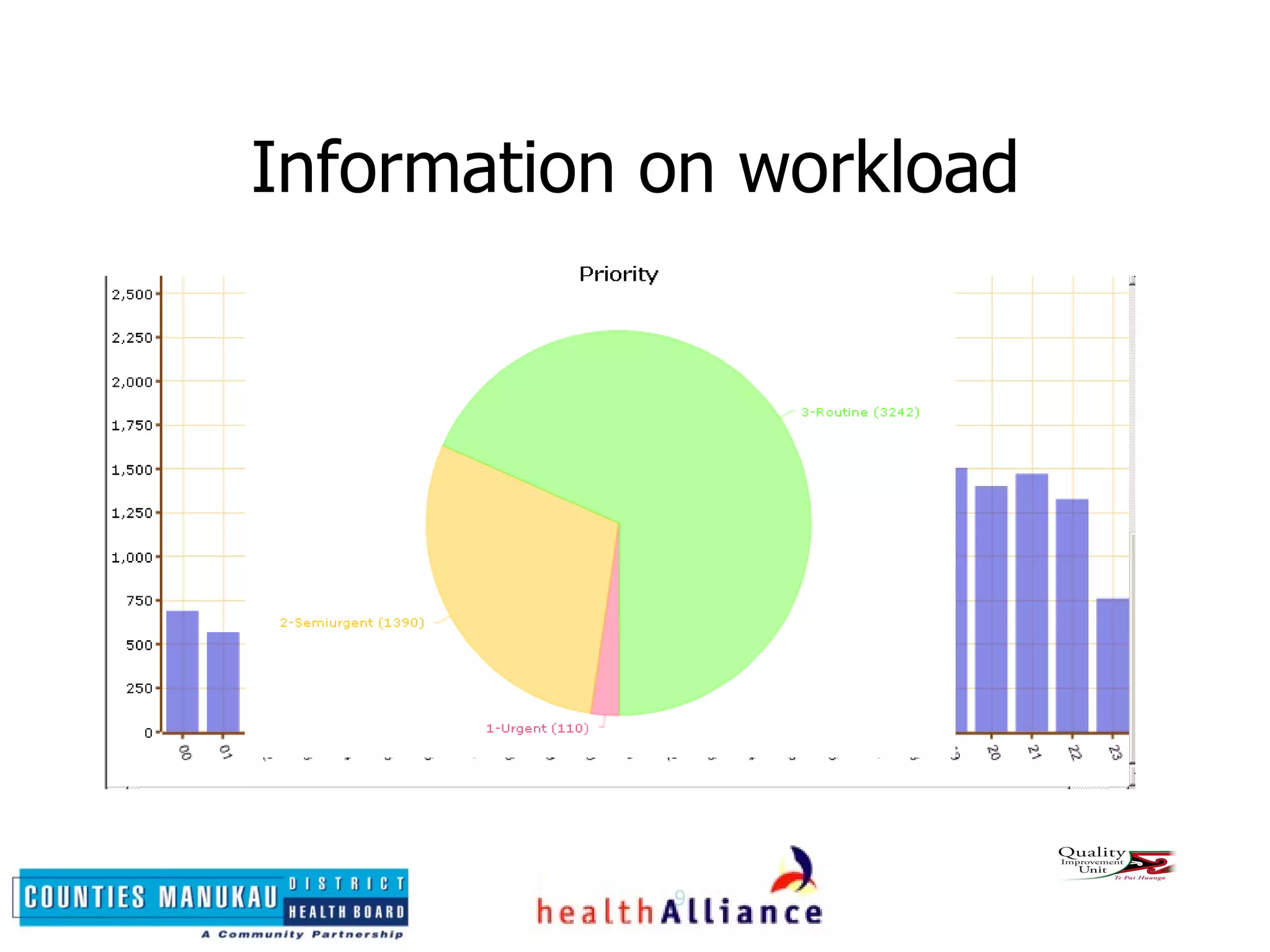
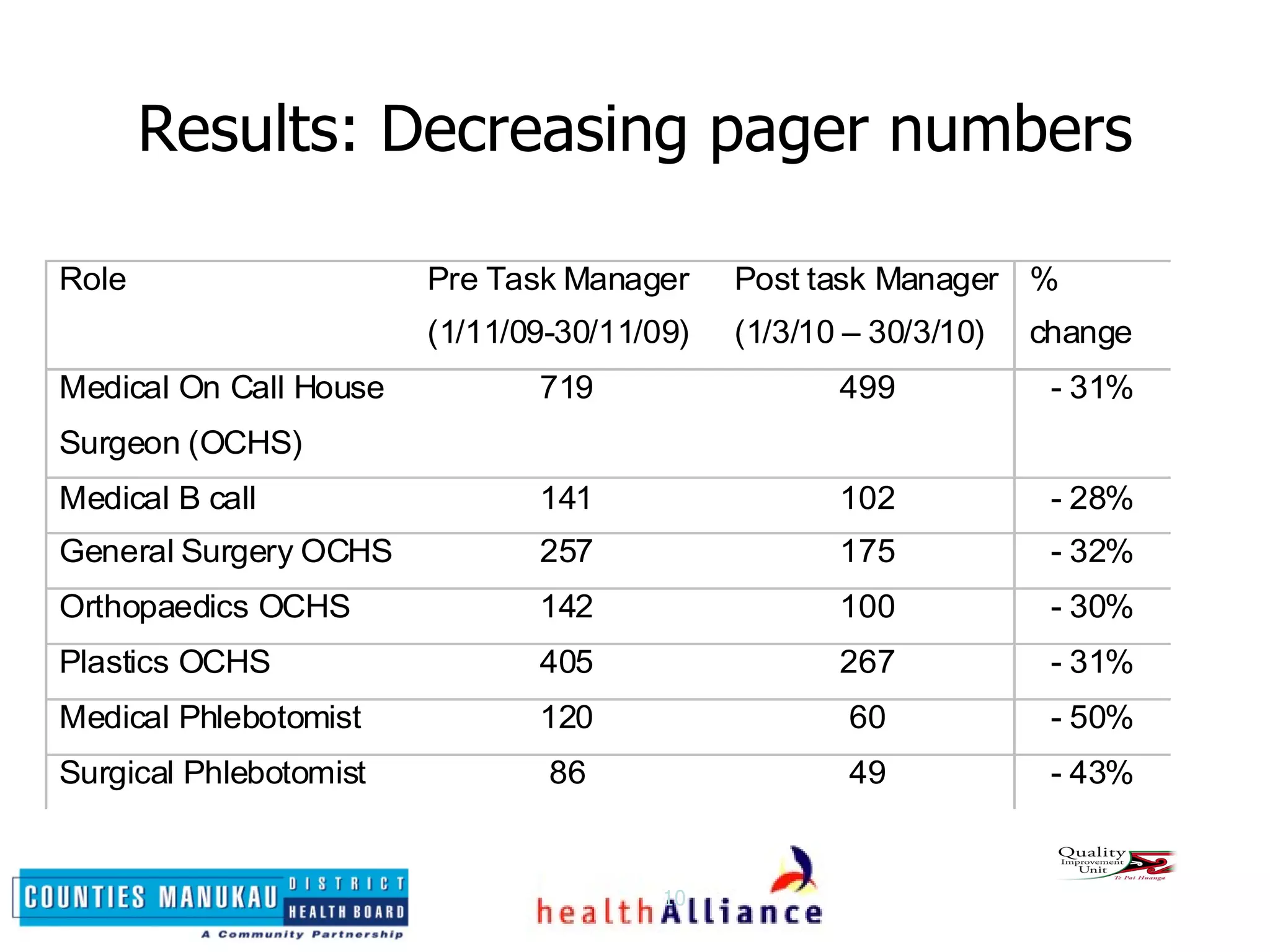
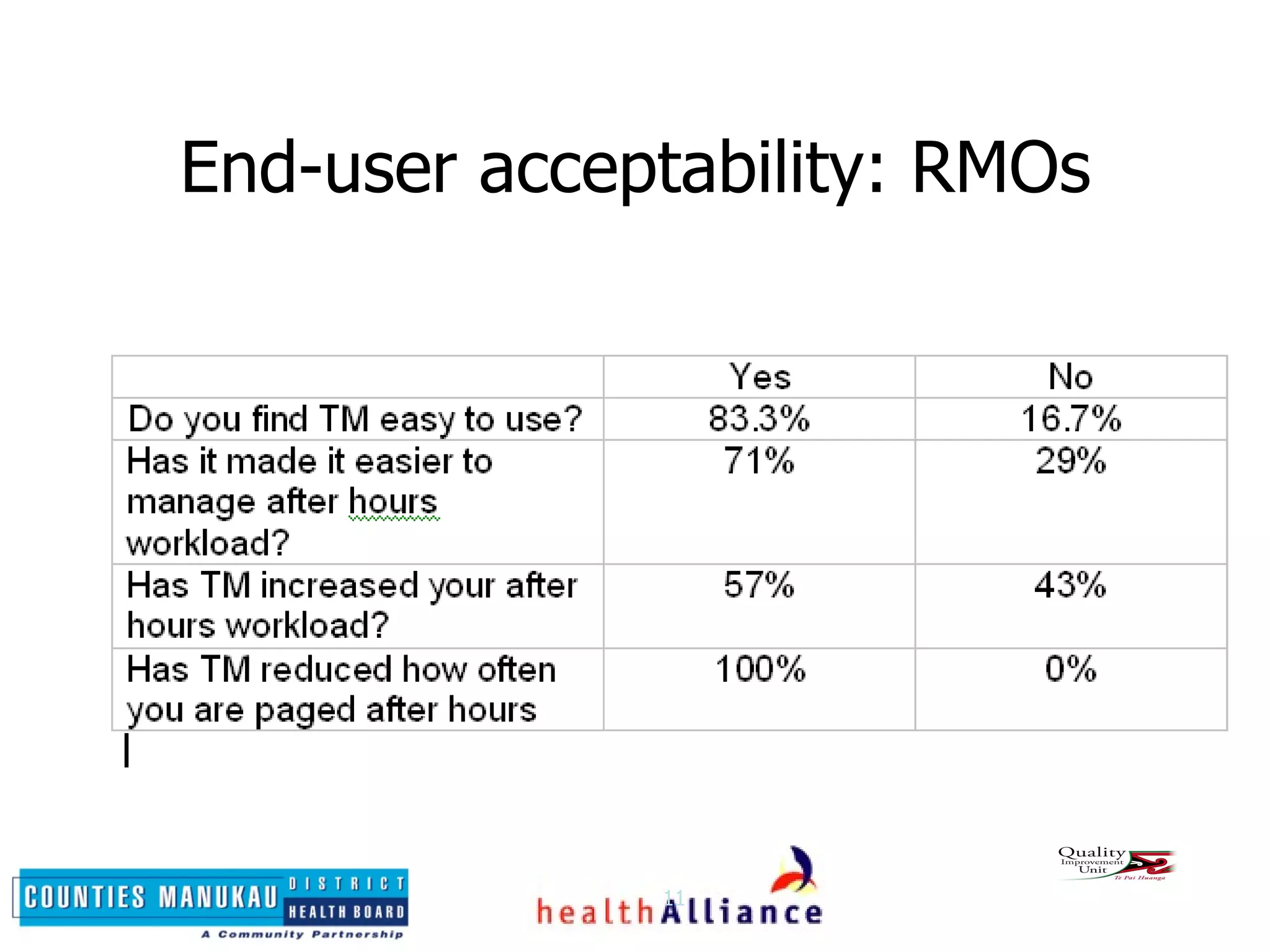
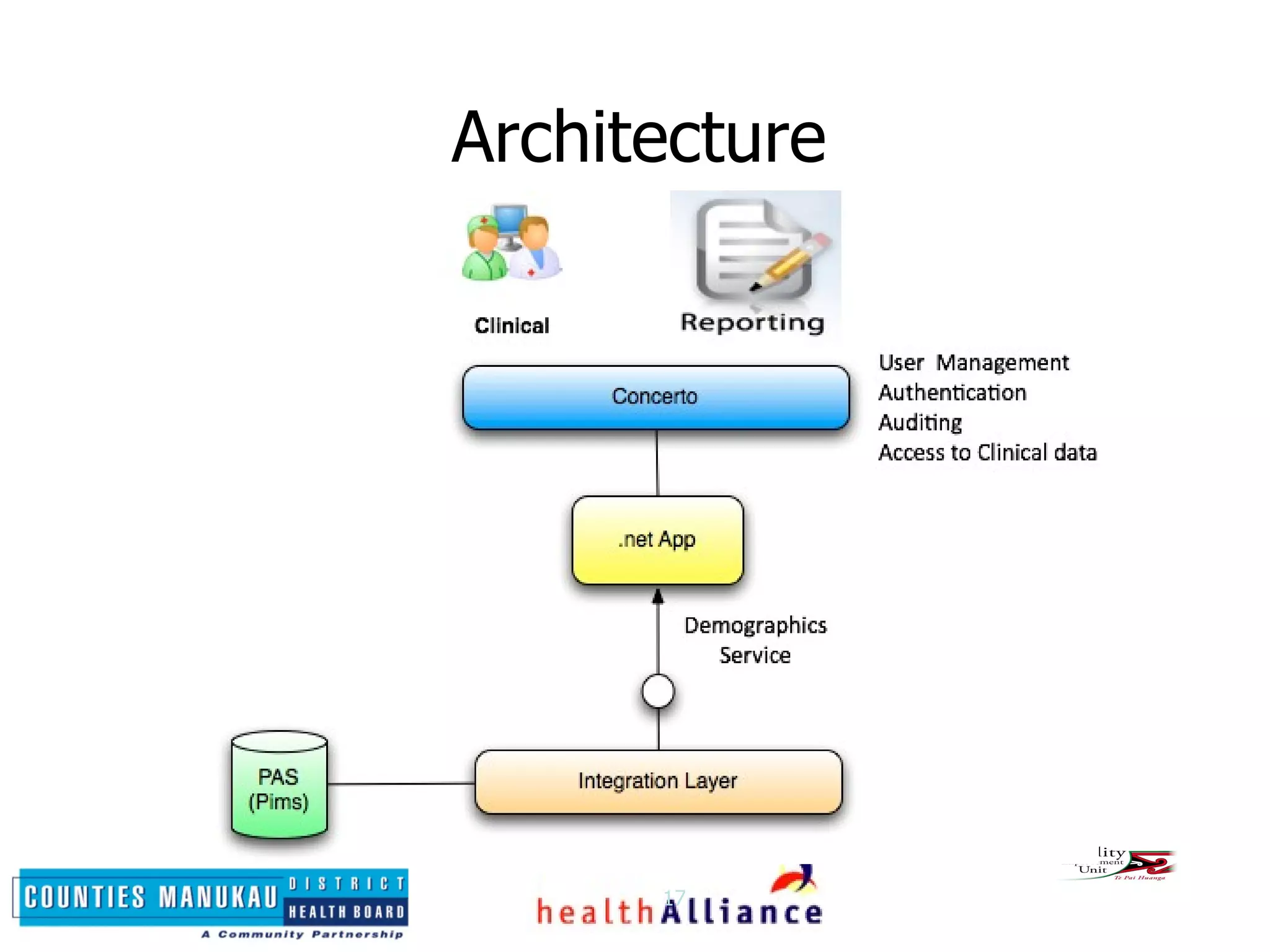

Task Manager is a digital application developed at Middlemore Hospital to improve communication between nurses and resident medical officers (RMOs) after hours. It allows nurses to create tasks and have them viewed, prioritized and accepted by RMOs from any computer. This provides visibility of workload and streamlines communication compared to pagers. Since implementing Task Manager, pager volumes have decreased and end-user surveys found it easy to use and improved communication. The application was inspired by another DHB's system but redeveloped internally to better integrate within their systems and support ongoing customization.






















































































