Downloaded 52 times




![REFERENCES
Avastin (bevacizumab) injection, solution [Genetech, Inc.]. US NLM, NIH, HHS.
Revised 01/2007.
<http://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?id=53695&CFID=6856876
5&CFTOKEN=c7cde62162e43be5-8E980C43-A853-F363-
B83B961222D86D50&jsessionid=ca301da0de303c387869>
Clinical Trials: Tamoxifen. US NLM, NIH, HHS.
<http://clinicaltrials.gov/ct2/results?term=tamoxifen>
Fisher B., Costantino J.P., Wickerham D.L., Redmond C.K., Kavanah M., Cronin
W.M., Vogel V., Robidoux A., Dimitrov N., Atkins J., Daly M., Wieand S., Chiu E.T.,
Ford L., and Wolmark N. 1998. Tamoxifen for prevention of breast cancer: report
of the national surgical adjuvant breast and bowel project p-1 study. Journal of the
National Cancer Institute. 90 (18). 1371-1388
Kleinsmith L.J., Kerrigan D., and Kelly J. 2010. Understanding cancer and related
topics: understanding esrogen receptors, tamoxifen, and raloxifene. National
Cancer Institute.
The Merck Index. 13th Edition. Merck & Co., INC. Whitehouse Station, NJ. 2001.
23](https://image.slidesharecdn.com/tamoxifen-140506144725-phpapp01/85/Tamoxifen-and-its-anti-cancerous-properties-23-320.jpg)
![REFERENCES
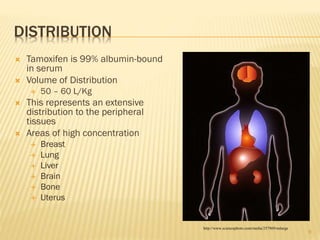
Lien E.A., Solheim E., and Ueland P.M. 1991. Distribution of tamoxifen and its
metabolites in rat and human tissues during steady-state treatment. Cancer
Research. 51. 4837-4844
Mackay H.J. and Twelves C.J. 2003. Protein kinase C: a target for anticancer
drugs.Endocrine-Related Cancer. 10. 389-396
Fisher B., Costantino J.P., Wickerham D.L., Cecchini R.S., Cronin W.M., Robidoux A.,
Bevers T.B., Kavanah M.T., Atkins J.N., Margolese R.G., Runowicz C.D., James J.M.,
Ford L.G., and Wolmark N. 2005. Tamoxifen for the prevention of breast cancer:
current status of the national surgical adjuvant breast and bowel project P-1 study.
Journal of the National Cancer Institute. 97 (22). 1652-1662
Nolvadex (tamoxifen citrate) Tablet [AstraZeneca Pharmaceuticals LP]. US NLM,
NIH, HHS. Revised 01/2007.
<http://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?id=3420>
24](https://image.slidesharecdn.com/tamoxifen-140506144725-phpapp01/85/Tamoxifen-and-its-anti-cancerous-properties-24-320.jpg)



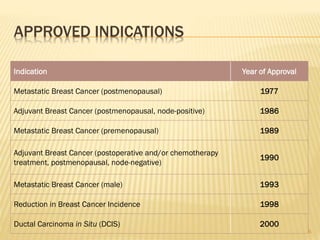
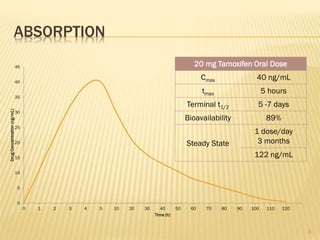
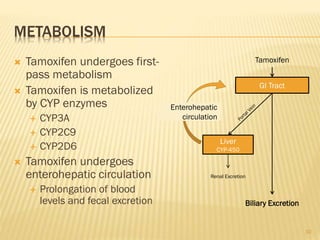
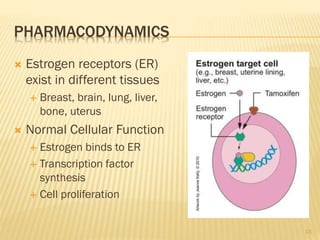
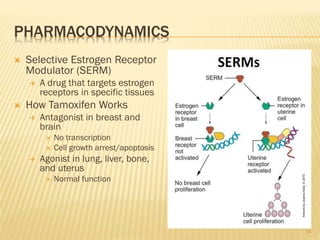
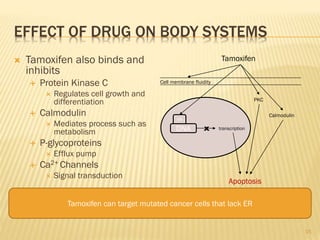
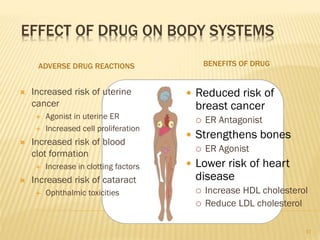
Tamoxifen is a selective estrogen receptor modulator originally developed as an antifertility drug. It is now commonly used to treat and prevent breast cancer. Tamoxifen undergoes extensive metabolism and is primarily excreted through the bile. It acts as an estrogen receptor antagonist in breast tissue to inhibit cell growth. A special population study found tamoxifen may also be effective for treating brain cancers due to its ability to inhibit protein kinase C and cross the blood-brain barrier.

















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















