Recommended
PPT
PPTX
การแก้ปัญหาด้วยกระบวนการเทคโนโลยีสารสนเทศ
PPTX
PPT
PPT
PPT
PPT
PDF
Selling Simplified Lead Care Solution Infographic
PPT
PPT
PPTX
การใช้งานโปรแกรม Microsoft Access
PPT
Hvidovre mediciner 2008 nov
PPT
PPT
PPT
PPTX
How Smart Business Intelligence Yields Rapid Association Growth
PPT
PPT
PPT
PPT
PPT
PPT
PPT
PPT
PPT
PPT
PPT
PPT
More Related Content
PPT
PPTX
การแก้ปัญหาด้วยกระบวนการเทคโนโลยีสารสนเทศ
PPTX
PPT
PPT
PPT
PPT
PDF
Selling Simplified Lead Care Solution Infographic
Viewers also liked
PPT
PPT
PPTX
การใช้งานโปรแกรม Microsoft Access
PPT
Hvidovre mediciner 2008 nov
PPT
PPT
PPT
PPTX
How Smart Business Intelligence Yields Rapid Association Growth
Similar to Sygeplejersker 2009
Sygeplejersker 2009 1. 2. Internationale kriterier for iltbeh.
PaO2 <7.3 kPa (Sat. 88%)
(7.3-8.0: EVF>55% or cor pulmonale)
Post-PaO2 >8.6 kPa
Stabile & optimalt behandlet
“Ikke-ryger”
Anvendt ilt >15 timer dagligt
Opfølgning/kontrol 1-3 mdr. Og sidenOpfølgning/kontrol 1-3 mdr. Og siden
halvårligthalvårligt
3. Effekt af iltbehandling
↓↓vejrtræningsarbejdevejrtræningsarbejde
↓↓åndenødåndenød
↑↑fysisk formåenfysisk formåen
↑↑hæmodynamikhæmodynamik ↓↓PAPPAP
↓↓Htc.: 4-8%Htc.: 4-8%
FEVFEV11: uændret: uændret
↑↑POPO22::
↑↑nyrefunktion (nyrefunktion (↓↓ødem)ødem)
↓↓trættræt
↓↓søvnsøvn
↑↑tænker klart (IQ)tænker klart (IQ)
↑↑QoLQoL
↑↑overlevelse:overlevelse: 22 →→ 4 år4 år
↓↓indlæggelse: 25%indlæggelse: 25%
4. Rygning og iltbehandling
Effekt? Formentlig
15-24 timer/dag? Ikke hvis storryger
Sikkert? Ikke hos alle
Etiske aspekter? Seretide til rygere?
5. 6. Formål med bærbar ilt
Iltmangel i hvile
↑timer med ilt
↑aktivitet evt. kommer på gade
Iltmangel under anstrengelse
↑fysisk formåen/mindre åndenød??
7. Akutte virkning af bærbar ilt
↓åndenød (Borg score 0.5-1.0)
↑Fysisk tolerance 5-20%
+
Vægt af udstyr
Risiko for falde i slangen
Ikke vise sig offentlig pga
generthed
-
8. Patient karakteristika
KOL: ca. 70%
Lungekræft: ca. 15%
Lungefibrose: ca. 5%
Hjertelidelse: ca. 5%
Neuromuskulær-lidelse/kyfoskoliosis: ca. 5%
Kvinder: ca. 60%
Flow: 1.4 L/min.
Alder: 72 år
9. Praktiske forhold ved LTOT
Hvordan ordineres LTOT?
Fugtet luft?
Pulssaturation versus a-punktur?
Sat.O2 ≥ 92%: stop
Sat.O2: 89-91: a-punktur
Sat.O2 ≤ 88: fortsæt
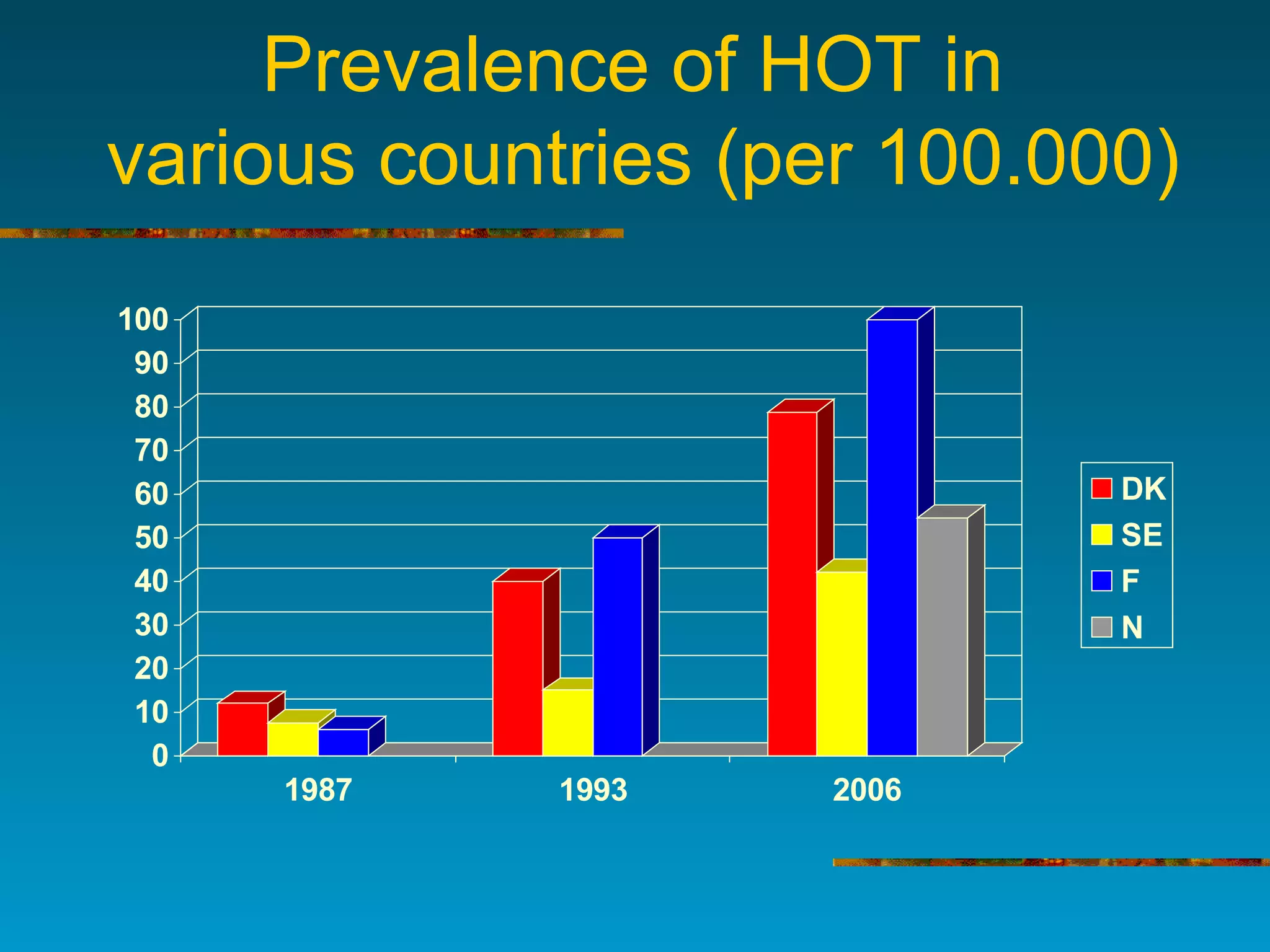
10. Prevalence of HOT in
various countries (per 100.000)
0
10
20
30
40
50
60
70
80
90
100
1987 1993 2006
DK
SE
F
N
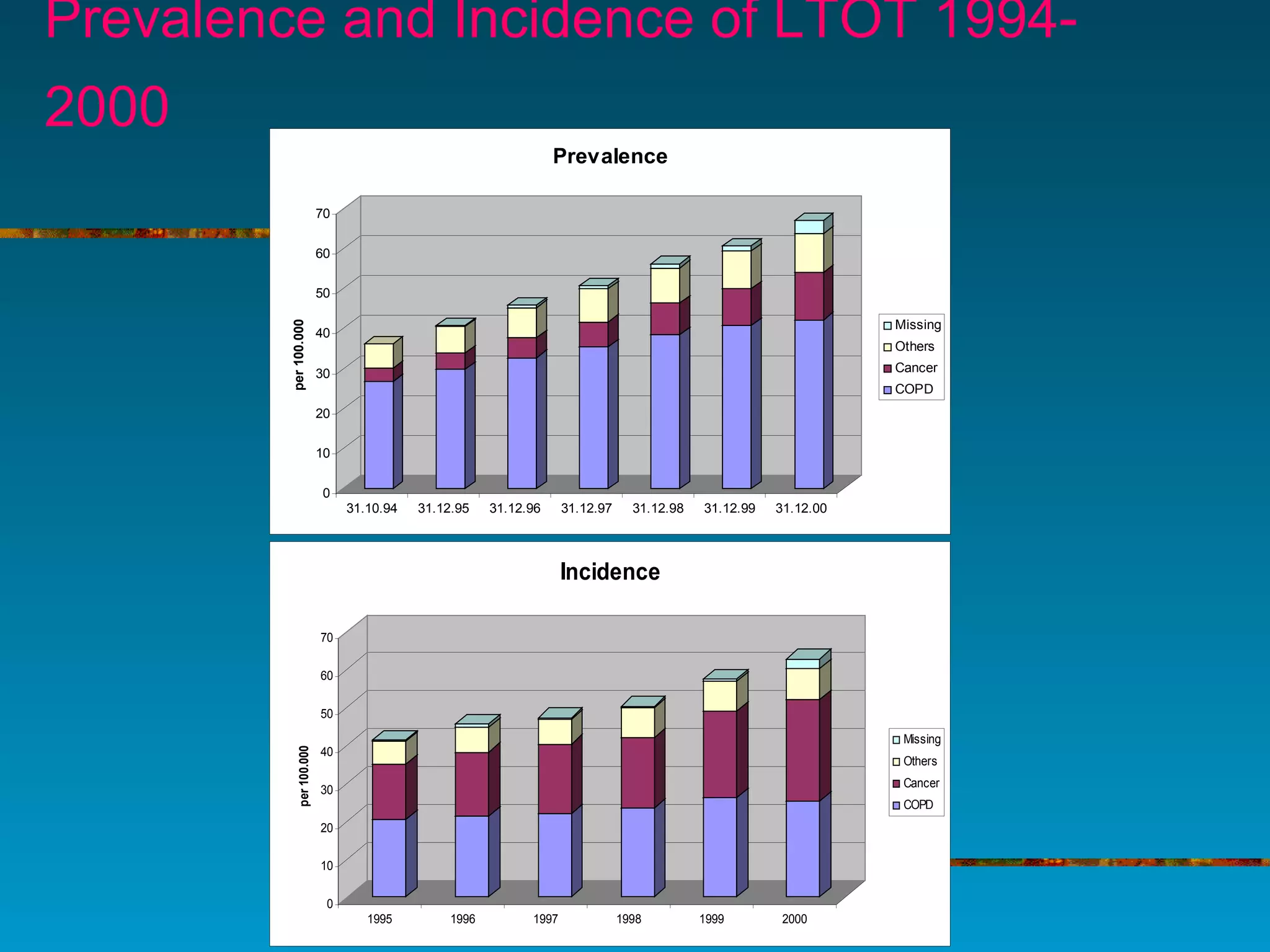
11. Prevalence and Incidence of LTOT 1994-
2000
0
10
20
30
40
50
60
70
per100.000
31.10.94 31.12.95 31.12.96 31.12.97 31.12.98 31.12.99 31.12.00
Prevalence
Missing
Others
Cancer
COPD
0
10
20
30
40
50
60
70
per100.000
1995 1996 1997 1998 1999 2000
Incidence
Missing
Others
Cancer
COPD
12. Konklusioner
Iltterapi ved kronisk iltmangel forlænger
overlevelsen og mindsker symptomer
De fleste patienter starter ilt efter indlæggelse,
og omkr. Halvdelen af disse har kun behov for ilt
midlertidigt (opfølgning vigtig!).
Bærbar ilt tungt og besværligt
Generelt høj dødelighed
13. Editor's Notes #12 In 1994 the prevalence of COPD was about 27/100.000. I the following years, it increased by about 50% to 42/100.000
The incidence of COPD increased from 20 to 25/100.00 during 5 years