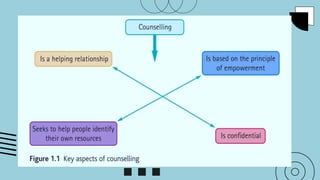
Topic outline
Interactionbetween Counseling and Social work
Counseling in social work helping process
Counseling in social work and client’s perspectives
Preliminary, beginning, action and ending phase
Qualities of an effective counselor
Counseling skills
Theories and approaches
Different therapies used by clinical practitioners
Kubler-Ross Emotional Reaction to problem
Social Work Counseling
-is a face-to-face communication in which one person (the counselor) helps
another (counselee) person make decisions based on a consideration of
alternatives, and acts on them (Mendoza, 2022).
Interviewing is the main tool to do counseling. It is also “a collaborative effort
between the counselor and the client. It helps clients identify goals and potential
solutions to problems which cause emotional turmoil.”
– Thelma Lee Mendoza
One of the key interventions to clients who have needs and problems.
Involves a purposeful and professional relationship between two parties –
the counselor and the counselee.
5.
Counseling
is aprofessional activity that involves helping clients individually or in
groups, or as couples and families, deal with various career,
vocational, educational, and emotional problems.
It is practiced by counselors, social workers, psychiatric nurses,
psychologists and psychiatrists.
It differentiates from psychotherapy for clients with mental illnesses
and psychological disorders.
6.
A plannedinteraction between the client and the worker to assist
client in altering his/her present behaviour.
Helps the client through guidance and support to find a solution to
a problem and make a decision.
To enhance the client’s ability to understand his/her situation and
adequately cope with the demands and challenges of life.
Counseling as anintegral part of
the Social Work Helping Process
Practice evolved to different areas
including behavioral, ecological, and
systems theories, and other practice
methods (Sedan 2001 and 2005)
Counselling service and the methods
used by counsellors became more
diverse. But Psychodynamic counselling
remained a major theoretical
approach.
The relationship between social work
and Counselling has always been
complex and interactive as these two
share some theoretical origins and ways
of thinking.
Counselors approaches were grounded
in Casework principles based on
psycho-dynamic theoretical
underpinnings.
9.
Counseling as anintegral part of
the Social Work Helping Process
At this time, boundaries between the
activities of social work and counseling
were not clear yet. Yet theory and
practice in the two areas of work
remain complementary.
Counselling practice has been re-
evaluated for its relevance in work with
people in crisis situation.
Counselling training, has examined its
ideologies and practices as society’s
attitudes and values have changed.
10.
Counseling as anintegral part of
the Social Work Helping Process
In reality, social workers in a number of situations take counseling roles, and
counseling (skills) or knowledge are applied to a number of social work tasks.
Various practitioners use counseling skills in the assessment and
implementation of services.
Presently, no known social workers are engaged in the private practice of
counseling in the country at this time. Social workers who engage in counseling
in the country function in an agency setting, and this is carried out usually in
conjunction with other approaches (Mendoza, 2022).
11.
The Barclay reportidentified counseling as one of the two main activities of social
workers, the other being social care planning,
- the report acknowledged the interlocking nature of these activities.
- challenge faced by social workers is to offer counseling in a way that is
integrated appropriately with a variety of other approaches in the overall work
with a given client often within the same interview
- This acknowledgment is affirmed in the social case work definition – one of the
three methods of social work.
Counseling as an integral part of
the Social Work Helping Process
12.
Counseling as anintegral part of
the Social Work Helping Process
Logical categorization of the counseling dimensions of social work according to
Brearley (1991):
Counselling skills underpinning the whole range of social work
Counselling as a significant component of the work, carried out in conjunction with other
approaches
Counselling as a major explicit part of the job description.
13.
Counseling vis-à-vis qualificationin
professional social work
National Occupational Standards for social workers and social work:
“A profession which promotes social change, problem solving in human relationships and the
empowerment and liberation of people to enhance well-being. Utilizing theories of human
behaviour and social systems, social work intervenes at the points where people interact with
their environments. Principles of human rights and social justice are fundamental to social
work.”(International Association of Schools of Social Work and the International Federation
of Social Workers)
14.
According to ThelmaLee Mendoza
- a practice-based profession and an
academic discipline that promotes social
change and development, social
cohesion, and the empowerment and
liberation of people.
SW as defined in RA 4373
- is the profession which is primarily
concerned with organized social service
activity aimed to facilitate and strengthen
basic social relationships and the mutual
adjustments between individuals and
their social environment for the good of
the individual and of society
15.
This international definitionprovides an ecological perspective which suggests social
workers are engaged with people who are themselves interacting with their environments.
Its aspirations are unlikely to conflict with the ethics of doctors, counselors or other
professionals with whom social workers collaborate, but social workers have a distinct role
in keeping a focus on people’s expressed needs, understanding the impact on people of
economic and social inequalities and offering social support.
16.
• Since theBarclay Report, Counseling h a s been mentioned a s a
function of social work … but it did not clarify its mea ni ng in relation to
social work.
• It is clear that social workers need to ha ve at least basic counseling
skills for communicating and relating. It is not necessary for all
social workers to be qualified for in-depth Counselling. W h a t i s
r e q u i r e d d e p e n d s u p o n t h e s e t t i n g w h e r e t h e s o c i a l w o r k e r i s
e m p l o y e d .
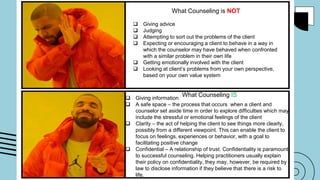
What Counseling isNOT
Giving advice
Judging
Attempting to sort out the problems of the client
Expecting or encouraging a client to behave in a way in
which the counselor may have behaved when confronted
with a similar problem in their own life
Getting emotionally involved with the client
Looking at client’s problems from your own perspective,
based on your own value system
Giving information
A safe space – the process that occurs when a client and
counselor set aside time in order to explore difficulties which may
include the stressful or emotional feelings of the client
Clarity – the act of helping the client to see things more clearly,
possibly from a different viewpoint. This can enable the client to
focus on feelings, experiences or behavior, with a goal to
facilitating positive change
Confidential – A relationship of trust. Confidentiality is paramount
to successful counseling. Helping practitioners usually explain
their policy on confidentiality, they may, however, be required by
law to disclose information if they believe that there is a risk to
life.
What Counseling IS
19.
The Helping Relationshipin Counseling
Counselor-client relationship is unique as it establishes a one-way relationship
with the purpose of resolving a concern and/or fostering the growth of one
person – the client
Counselor is designated as the helper and expected to have the knowledge &
training to assist the client in an intentional and systematic way.
20.
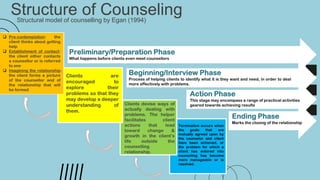
Structure of Counseling
Structuralmodel of counselling by Egan (1994)
Preliminary/Preparation Phase
What happens before clients even meet counsellors
Beginning/Interview Phase
Process of helping clients to identify what it is they want and need, in order to deal
more effectively with problems.
Action Phase
This stage may encompass a range of practical activities
geared towards achieving results
Ending Phase
Marks the closing of the relationship
Pre-contemplation: the
client thinks about getting
help
Establishment of contact:
the client either contacts
a counsellor or is referred
to one
Imagining the relationship:
the client forms a picture
of the counsellor and of
the relationship that will
be formed
Clients are
encouraged to
explore their
problems so that they
may develop a deeper
understanding of
them.
Clients devise ways of
actually dealing with
problems. The helper
facilitates client
actions that lead
toward change &
growth in the client’s
life outside the
counselling
relationship.
Termination occurs when
the goals that are
mutually agreed upon by
the counselor and client
have been achieved, or
the problem for which a
client has entered into
counseling has become
more manageable or is
resolved.
21.
Characteristics of PositiveHelping relationship
(Seligman 2004)
Provides a safe and protective environment for clients;
Encourages collaboration, with both clients and the helpers playing an
active role in the counselling process;
Mutual feeling of shared warmth, caring, affirmation & the respect;
Client and counsellor have an agreement on goals an procedures;
sessions are structured in such a way as to clearly move toward
accomplishment of these goals;
Client & counsellor view themselves as engaged in a shared endeavor
that seems likely to succeed.
22.
Types of Counseling
Acounselling which usually concentrate
on helping a person around the time of
crisis, and can only take place when
there is a possibility for interpersonal
interaction.
01
Crisis Intervention
Counselling
A counselling devoted toward stopping
something before it develops. Risk of
developing the behaviour is identified,
effort is given in trying to stop further
development.
02
Preventive
Counselling
It is structured., involving active empathetic
listening to help individuals to identify problems,
analyze them and find alternative solutions.The
aim is to help clients to accept circumstances
and to reduce adverse effect of the problem
in his/her psychosocial well being.
03
Problem-Solving
Counselling
Usually works well after a problem-
solving process has taken
place when the client is facing the
risk of making difficult decisions
04
Decision-making
Counselling
23.
Types of Counseling
Avery common form of one-on-one counselling. Some problems are very personal and difficult to
confront with other people around.
05 Individual Counselling
Theory
- is theset of empirically testable, interconnected ideas formulated to explain
those phenomena (Doherty, Boss, LaRossa, Schumm, & Steinmetz, 1993;
White & Klein, 2002).
26.
The Psychodynamic Approach
Thisapproach to counselling stems from the work of Sigmund Freud
(1856–1939). Ideas that are central to psychodynamic theory include
those of unconscious motivation, psychosexual stages of development,
innate sexual and aggressive drives, links between childhood and present
behaviour, and the nature of defense mechanisms and their use.
27.
The Psychodynamic Approach
Isone of the contemporary approaches concerned to help clients identify the
often hidden (or unconscious) factors that can influence behaviour.
- is that early experiences are seen as important in shaping the way our mind
works.
- tries to help clients understand long-standing conflicts from the past which
helps the client become more self-aware and bring what is unconscious into
consciousness.
- It focuses on the fact that many of the personal troubles in life
are the result of mental processes that are hidden from us.
28.
The Social PsychologicalApproach
• method that focuses on the encounter between an individual and the
environment in which he/she operates.
• Asserts that individual’s thoughts, feelings, and behaviors are influenced by
social situations.
• Focuses on how one construe or interpret situations and these interpretations
influence their thoughts, feelings and behaviors (Ross & Nisbett, 1991);
• concerned with creating and uncovering resources within the individual, with
the goal of helping the individual reach a functioning level that is more
satisfactory and complete.
29.
Adler disagreed withFreud’s emphasis on the sexual instincts and biological determinism
as the basis for human behaviour. He asserts that a person is a product of his past
experiences as he/she develops personality in stages based on environment and
relationships with family and community.
This approach influenced psychosocial counselling. It provides a framework of resources
from which psychosocial counselling draws when dealing with diverse problem situations
that affect people in their social lives.
How does this approach work in social work practice and counselling?
The Social Psychological Approach
30.
The Goals ofthis Approach (specifically with psychosocial approach):
• Reducing distress experienced by the individual.
• Enhancing the individual’s personal well-being.
• Recognizing and marking problem areas and the actions that are needed in order to change the situation.
• Identifying coping resources, strengths and capacities inherent within the individual for coping with the problem
at hand.
• Creating optimal compatibility between the individual and his/her physical and social environment.
Intervention Methods of the Psychosocial Approach:
• Focusing on the “here and now”: examining the individual’s behavior, emotions and thoughts in the context of
the problem being coped with, while utilizing the relationship with the therapist as a touchstone.
• Observation of dynamic patterns: identifying beliefs, thinking patterns and emotions which have become
engrained in the individual and that may influence the problem.
Developmental observation: reference to the individual’s family of origin and to early experiences which
influence the personality and the current functioning of the individual.
The Social Psychological Approach
31.
This approach tocounselling is based on the work of a group of behavioural
psychologists who were interested in the nature of human learning.
Aaron Beck is the father of CBT in the 1960’s other behavioural psychologists
include Pavlov (1849–1946), Watson (1878–1958) and Skinner (1904–1990).
An evidenced-based kind of therapy that has been proven effective to treat
behavioral problems of numerous kinds.
The Cognitive Behavioural Approach
32.
The Cognitive BehaviouralApproach
- Short-term goal on a psychotherapy.
- views human personality as a collection of learned behaviours.
- as its title implies, concerned with a person’s thinking and the way in which it affects his or her
behaviour. This approach extends and enhances the purely behavioural facets of the person,
almost exclusively concerned with learned behaviours and the observation of behaviour.
- The goal is to change the negative pattern of thought and behaviors
that are behind people’s difficulties.
- Helpful in a range of problems e.g psychological problems, anxiety, depression,
marriage and relationship problems
33.
CBT approach usuallyinvolves efforts to change thinking patterns which
include:
• Learning to recognize one’s distorted thoughts that are creating problems
and then reevaluate them in light of reality
• Gaining a better understanding of the behavior and motivation of others;
• Using problem-solving skills to cope with difficult situations;
• Develop a greater sense of confidence in one’s own abilities – involves
efforts to change behavioral patterns by facing one’s fears, using role
playing, learning to calm one’s mind and relax one’s body.
The Cognitive Behavioural Approach
34.
Another modality onCBT is the Behavior Modification. Maladaptive behaviour can be perpetuated
through reinforcement, so a focus of behaviour therapy is identification of the ways in which problem
behaviour is maintained. When this identification is made, techniques can be used to change the
problematic stimulus–response pattern.
- Positive and negative reinforcements
- Positive and negative punishments
Core Principles:
- Problems are based on faulty or unhelpful behavior.
- Problems are based on learned patterns of unhelpful behavior
- People suffering psychological problems can learn better ways of coping with them
The Cognitive Behavioural Approach
35.
The Humanistic Approach
Personalityis seen as unique to the individual, and problems are set in the
context of each person’s unique experience.
The humanistic approach works on the concept that human nature is
inherently good and everyone has the potential to find their own answers to
their problems. Here Adler applies Maslows theory of motivation using the
premises of the Hierarchy of Needs.
The humanistic approach is about free will, self-discovery and achieving your
full potential as a human being, rather than concentrating on individual
problems or symptoms. It looks at everything that makes you who you are
and focuses on you as a unique individual and your relationship with the
world around you.
36.
The Humanistic Approach
Humanistictherapy is client-led, therapist works in exploring the issues.
Counselors help clients think about their feelings and take responsibility
for their thoughts and actions.
Helps clients think about their feelings and take responsibility for their
thoughts and actions.
Therapy may be short or long-term, depending on the client’s needs.
37.
The Humanistic Approach
Isan umbrella term that covers several types of therapy, including
Person-centered therapy, Gestalt, existential therapy, solution-focused
therapy and transactional analysis.
Important names in the humanistic tradition include Carl Rogers
(1902–1987), Abraham Maslow (1908–1970) and Fritz Perls (1893–1970).
38.
Humanistic psychology arguesthat each human being is a unique and complex
individual, who has potential and responds to more than punishments, rewards, and
urges. Learn about the humanistic movement in psychology, and explore Abraham
Maslow's contributions.
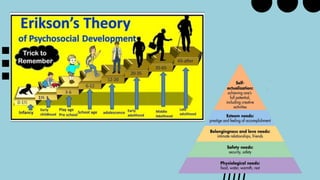
Maslows Pyramid of needs or Erickson’s Psychosocial Stages of Development - a person’s
motivation lies in the level of the hierarchy/stage that they are currently pursuing.
Painful and difficult life events can block a person’s self-belief and worth, and obscures their
ability to find solutions and emotional freedom.
The humanistic approach works on gently removing these blocks allowing constructive and
healthy emotional and psychological growth
40.
- is aboutfree will, self-discovery and achieving your full potential as a human being,
rather than concentrating on individual problems or symptoms. It looks at everything
that makes a person who they are and focuses on the person as a unique individual
and their relationship with the world around them.
Alfred Adler’s Personality Theory diametrically opposed (in terms of ideology) to
both the psychodynamic and behavioral traditions. This is because the humanistic
view emphasizes the innate potential every person is believed to possess.
41.
1. Directive orCounselor –Centered - focused on the problem
than the person, counselor lead the problem-solving
process.
2. Non-directive or Client-Centered – client takes the lead and
active role. Free expression of situation, counselor directs,
guides and decides of the working relationship
3. Eclectic Counseling – client and the counselor work
collaboratively using a mix of the two approaches.
Mendoza’s Approaches to Counseling
Ethical Considerations
The word‘ethics’ refers to the study of right and wrong behaviour, and in
the counselling context this has special relevance. This is because of the
close nature of the therapeutic relationship and the possibility of abuse
that exists within it.
44.
Ethical Considerations
Confidentiality
In thecontext of counselling, the word ‘confidentiality’ means ensuring that what is
told in ‘confidence’ by a client is not repeated to anyone else, apart from certain
exceptional circumstances. It is often seen as an absolute right for clients who,
after all, trust counsellors with some of their most intimate thoughts, feelings and
desires.
The information clients disclose in counselling may never have been spoken to
anyone before and, indeed, it often takes clients a very long time to summon up the
courage to approach helpers in the first place. For this reason, clients need to have
confidence in the professional integrity of helpers and in their ability to keep private
anything they discuss.
45.
Ethical Considerations
Confidentiality
The followingare some general guidelines relating to confidentiality.
1. Confidentiality is a subject that needs to be addressed as early as
possible in counselling, although in crisis situations this may not be
immediately feasible.
2. Even in crisis situations the issue of confidentiality should be
addressed at some stage.
3. An atmosphere of trust is just as important as an explicit statement of
confidentiality.
46.
Ethical Considerations
Confidentiality
Some Limitationsinclude:
1. Exceptional circumstances-include urgent and serious situations, such
as threats of harm to self, or others, by a client.
2. Client’s information is pooled in situations where helpers work closely
together, but even here clients must be informed about (and agree
to) this practice
3. Guidelines stated by a particular counselling agency or organisation,
cannot remain confidential.
Ethical Considerations
Confidentiality
Talking aboutClients:
There are frequent discussions about problems encountered in
professional work. The usual practice is to refer to clients indirectly and never by
name. It is difficult to see how ideas and issues can be shared without these
discussions, but there is a case for saying that every casual reference to clients,
however indirect, is bound to devalue the integrity of the counsellor–client
relationship to some extent, at least.
49.
Ethical Considerations
Confidentiality
Talking aboutClients:
We all need to be circumspect when talking about work, because even
though clients have no knowledge of these discussions, the effects of the way the
counsellors treat them behind their backs do manifest during counselling. Weinberg
(1996: 68) highlights this phenomenon and points to the possibility of the therapeutic
‘alliance’ being weakened as a result of this indirect loss of confidence. In other words,
clients do pick up unconsciously transmitted messages during counselling, and when
these attitudes convey casual attitudes about confidentiality, real trust will never
develop.
50.
Ethical Considerations
Confidentiality
The Client’sResponsibility:
Another aspect of confidentiality concerns the client’s obligation (if any)
towards maintaining it. The issues should be discussed early in the first session
with the client. When clients find the request for confidentiality difficult in some
respect, then the difficulties are explored and discussed too. There are probably
quite a few clients who would, in fact, experience anxiety if requested to make a
pledge of confidentiality in counselling. These include people who have been
traumatised in childhood, as a result of keeping ‘secrets’ relating to sexual or other
forms of abuse.
51.
Ethical Considerations
Transference andthe Counselling relationship
Transference refers to the client’s emotional response to the counsellor
(or to any other helper) and that it is based on much earlier relationships,
especially those formed in childhood with parents and other important
people in the client’s life. When people are distressed they are,
of course, vulnerable and this vulnerability makes them open to abuse,
however unintended.
52.
Ethical Considerations
Transference andthe Counselling relationship
Unconscious feelings
Unconscious transference feelings can be positive or negative, distrustful,
idealising, loving, erotic, envious or antagonistic. Though these (and many
other possible responses) may not be obvious at the beginning of
counselling, they tend to emerge once the client–counsellor relationship is
established. When Freud first wrote about psychoanalysis, he described it
as ‘the true vehicle of therapeutic influence’ (Freud, 1909: 84). He also
added that the less transference is suspected by a therapist, the more
likely it is to operate in a powerful way (Freud, 1909).
53.
Ethical Considerations
Transference andthe Counselling relationship
The word ‘countertransference’ describes the counsellor’s emotional
response to the client’s transference. A counsellor who is, for example,
cast in the role of critical parent, may well be drawn into responding in the
way that a critical parent would respond. This type of unconscious role
play situation may continue unproductively and indefinitely, unless and
until it is identified and changed either through spontaneous insight, or
with the aid of supervision.
54.
Ethical Considerations
Transference andthe Counselling relationship
Lack of objectivity
Any distorted view of the client–counsellor relationship will inevitably get
in the way of objectivity when working with clients and their problems.
When counsellors experience countertransference feelings towards
clients, they need to be able to ‘contain’ these, rather than acting on them
in a way that clients act on their transference feelings.
55.
Ethical Considerations
The possibilityof exploitation
This emphasizes the point that counsellors need to know how to take care of their
own needs without involving vulnerable clients. Some of the other possible areas of
abuse within counselling and therapy include the following:
● failure on the counsellor’s part to undertake adequate supervision
● arriving late for sessions, or leaving early
● encouraging clients to become dependent
● being unclear or inconsistent about financial arrangements if these apply
● premature termination of counselling, and lack of consultation with clients
● failure to maintain confidentiality, or failure to inform clients if there is a
conflict of interest in relation to confidentiality.
56.
Ethical Considerations
Contracts
Establishment ofa contract, preferably in writing, ensures that both client
and counsellor understand the nature of the commitment between them
and what it entails. It helps to provide explicit and clear guidelines for
clients. Contracts are an essential component of all approaches to
counselling and should be made at an early stage. In the first instance, it
is useful to clarify certain points with clients, especially those relating to
the nature of counselling itself.
57.
Ethical Considerations
Contracts
The followingare important aspects of counselling, which clients should
be informed about from the outset:
● Confidentiality and its limitations
● Details regarding frequency and length of sessions and where these will
take place
● Financial terms if these apply, and how payments should be made
● Arrangements concerning missed appointments
● Details about holidays
58.
Ethical Considerations
Contracts
The followingare important aspects of counselling, which clients should be
informed about from the outset:
● Information about the counsellor’s qualifications, accreditation, supervision
and training
● Information about the counsellor’s approach and any specific procedures
likely to be used
● Details about regular reviews of progress between client and counsellor
● Discussion about ending counselling and how this will be manage
59.
Ethical Considerations
Contracts
The followingare important aspects of counselling, which clients should be
informed about from the outset:
● Details about record-keeping by the counsellor and the client’s right to see
these
● Information about making a complaint, and procedures for clients to follow if
they wish to do this.
60.
Ethical Considerations
Ending Counseling
Theending of any relationship is obviously much more difficult for someone
who has lost a parent in early life, for example, or indeed for anyone who has
been bereaved in later life too.
Counseling be difficult for all of us and clients in counselling are no exception
in this respect. Many people experience a variety of conflicts about endings in
general, and this is especially true of those people who have been traumatized
by separations in the past.
61.
Ethical Considerations
Other Indications
Followinga successful experience of counselling, clients may continue their
own internal dialogue, similar to that conducted with the counsellor. In
addition, readiness to end counselling may also be indicated in other
significant ways. The client is likely to feel more independent, for example, and
as a result of this independence will see the counsellor as a ‘real’ person,
rather than an object or a transference figure. Increased understanding of ‘self’
is another aspect of client development, and often clients will demonstrate
more assertive attitudes as a result of this.
62.
Ethical Considerations
Other Indications
Fromthe counsellor’s point of view, this change is often ‘felt’ in the sense that
the client’s transference is no longer experienced and the counsellor becomes
more relaxed. When client and counsellor actually do separate, they do so as
equals who have worked together towards a goal (Solomon, 1992).
63.
Ethical Considerations
Referral
Clients maybe helped by people who work in a variety of helping occupations,
many of whom would not describe themselves as counsellors. One of the
difficulties that helpers may have, as a result of these trends, is to determine
the limits of their own capabilities in providing the right support for clients. An
important aspect of training, therefore, is identification of specific problem
areas that might require other forms of help or support.
64.
Ethical Considerations
Referral
Routine referralsto other services or agencies ‘should be discussed with the client in
advance’ (BACP, 2013). It adds that the client’s consent should be obtained before
making the referral; in addition, client consent should be obtained in relation to any
information that will be disclosed in the process of referral. It is also important to ensure,
as far as possible, that the referral is appropriate for the particular client, and that it is
likely to be of benefit to that client.
Clients should be given the opportunity to discuss their feelings about the prospect of
referral too. If they are not given this chance to express feelings, they may experience
resentment or anger in relation to the whole process.
65.
Ethical Considerations
Referral
Reasons forReferral
At every stage of the counselling process, helpers need to ask themselves what is the
best course of action for specific clients. The reasons for referral are obviously very
varied. Whatever the circumstances, and regardless of the problem, it is essential that
clients are given the opportunity to participate in any decisions made about them.
The counsellor’s task is to inform clients about any specialized services that are
available to them; it is then up to the client to accept or decline.
66.
Ethical Considerations
Referral
Resources forReferral
Preparation is probably one of the most important aspects of referral. All helpers,
including those whose work is part of other occupational responsibilities, need to be well
informed about all the resources available to them within the community and, indeed,
beyond. The names, addresses and telephone numbers of other professional workers
who might be in a position to help clients with specific needs should be kept on record.
Good liaison and consultation with other professionals is essential too. Continuing
education has the added advantage of keeping counsellors in contact with as many
people as possible, either locally or nationally, who may be able to help clients.
Principles
Acceptance
A guiding principleof the client-worker relationship which is characterized by
the worker’s recognition of the individual’s worth as a human being with
strengths as well as weaknesses, his/her congenial and uncongenial
qualities. It does not include antisocial attitudes and behavior.
69.
Principles
Communication
Communication should beverbal as well as non-verbal
and should be skillful particularly in disposing interviews in
order to come up concrete assessment and intervention
appropriate for the client’s needs or situation.
70.
Principles
Empathy
The worker’s abilityto put himself/herself in the shoes of the client so that
she/he can understand what the latter is thinking and feeling about her//his
problem or situation
71.
Principles
Non-judgmental Attitude
The workerrefrains from adopting a condemnatory attitude towards
the client’s behavior, past or present although he/she may take note
of it professionally.
- based on the conviction that the worker should not judge the client
on the basis of the problem and circumstances of the client.
72.
Principles
Confidentiality
The preservation ofsecret information concerning the client which is disclosed
in the client-worker relationship. This may not be divulged without the client’s
permission or that of pertinent authority and only for a specific purpose – for
the benefit of the client.
- In social casework, the principles of keeping the information confidential is
the right of the client and the duty of the social worker. It is an ethical practice
and obligation of the social caseworker.
- When or why sometimes confidentiality be reconsidered?
73.
Principles
Individualization
The recognition thateach person is unique, separate, and distinct from the
others and should be treated as such. This imply that no two person are alike
and so must receive counseling services suitable for their needs and
problems.
74.
Principles
Controlled Emotional Involvement/ProfessionalNoninvolvement
Refers to the worker’s way of reacting to the client’s purposeful expression of
feelings and implies professional detachment. It means that although the
worker must be empathetic, she/he must guard against becoming emotionally
involved with his/her client as this will likely color what should be an objective
viewpoint; usually taking side of the client. The worker in counseling is
therefore advised to remain neutral but sensitive, understanding, and
responsive.
75.
Empathy –understanding a person with an intent to
understand his unique situation and feeling; sensing
accurately the client’s world, seeing the way the client
does and verbally sharing his understanding
Respect and Positive Regard – Appreciate the client
as unique individuals regardless of who they are.
Genuineness – Honesty; shedding one’s expected role
or image, does not use disguises of mechanical
responses to fool or manipulate client. Is appropriately
spontaneous, non-defensive, open, and congruent in
thoughts, feelings, and action.
Concreteness – Accurate, clear, and specific
Qualities of an effective Counselor
76.
Trained, andGood Communicator– Professionally trained:
produce a counselee who will be autonomous and not
dependent.
Strength to do Counseling – Counseling is “emotionally
demanding”. it Is important for the counselor to be emotionally
stable.
Supportive of Another Person – Gives the client the
opportunity to talk encouraging opinions, describing anxieties
and fears without concern for verbal retaliation or rejection
Sense of Humor – Helps client to become relaxed and enjoy
the incongruities in his environment and the foolish aspects of
his behavior
Qualities of an effective Counselor
77.
Qualities of aneffective Counselor
• Interpersonal skills - be able to express themselves clearly and effectively. It is
important not only to be able to educate clients about therapeutic
topics, but also to gauge the client’s understanding at any given
time.
• Trustworthy - must be able to communicate verbally and nonverbally that they
are trustworthy. Having faith in the quality of the relationship and
the confidentiality of what is disclosed leads to a deeper
connection.
• Flexible - create a meaningful treatment plan that is individualized for each client.
Counselor shouldn’t follow a rigid schedule of treatment or have a “one
size fits all” approach. Be able to identify when treatment is not suitable
to the client.
78.
Qualities of aneffective Counselor
• Self- awareness - can separate personal issues from those of the client.
Determines occurrence of dilemmas, counter transference, and
its limitations.
• Hope and optimism – find a balance between realism and hope. Sets realistic
goals.
• Multiculturally Sensitive - it is important to be educated and sensitive to issues
of race, gender, ethnicity, sexual orientation, religion,
and cultural background.
79.
Qualities of aneffective Counselor
(Click photo to play the video)
80.
Verbal
Advising
Excessreassuring
Blaming and judging
Encouraging dependence
Interrogating
Keeping
Non-verbal
Keeping a distance
Using unpleasant tone of voice
Frowning
Speaking too fast or too slow
Non-supportive Behavior of
Counselor
Basic Counseling Skills
Activelistening/responding skills
Paying full attention to the client’s verbal disclosure,
non-verbal cues and feelings. Maintaining and
communicating active involvement with the client while
listening through non-verbal communication such as
eye-to-eye contact and nodding of the head.
- Involvement of the worker is measured not by the
number of words spoken or the issue covered, but by
the time he/she spends actively listening.
83.
Basic Counseling Skills
Paraphrasing
–Is restating the client’s message.. Making sure that the
client has understood what the worker just said & vice
versa. This will encourage the client to continue
speaking. ( example… I heard you say you are worried
about your son’s behaviour…is that correct? )
84.
Basic Counseling Skills
Clarifying
–Is making an educated guess about the client’s
message for the client to confirm or deny…. It is also to
clear up confusion if a client’s response is vague or
not understandable. (Example: I don’t think I
understand what you said..can you explain ….)
85.
Basic Counseling Skills
Askingappropriate questions… to obtain specific
information
- Asking the right question at the right time and the right
way will encourage client to communicate, elaborate on
his/her thoughts, knowledge or feelings; and to make
the client feel that the worker is interested in what
he/she has to say.
86.
Basic Counseling Skills
Askingappropriate questions… to obtain specific
information
- Open ended questions ..requires client to express his/her
feelings, beliefs, knowledge & gives more than a yes or no
answer. (what and how questions)
- Probing questions… helps the worker to clarify the client’s
response to open-ended question. Normally, probing
questions follow open-ended questions.
- Closed questions … usually Yes and No response or a
few words. It may discourage discussion or exploration.
87.
Basic Counseling Skills
Identifying& reflecting feelings
– help client identify and clarify ideas, feelings and reactions by
listening to how the feelings are described.
Problem clarification
- allowing the client to state the problem and help the client
clarify and define it. The social worker should not make
assumptions on what the client’s problem is, nor should worker
make an attempt to solve the client’s problem, solving it for
him/her.
88.
Basic Counseling Skills
Focusing
-help the client focus on the most important
issues at hand and not get side- tracked.
Appropriate use of silence
- Silence in counselling session is important. It
gives the client an opportunity to reflect, integrate
feelings, think through an idea or absorb new
information.
89.
Basic Counseling Skills
Providinginformation
– presenting information in a clear, concise and
understandable manner at a point in the session
in which it is appropriate and helpful.
Rephrasing statements for accuracy of
feelings expressed by the counselee.
- Giving honest feedbacks on messages.
90.
Basic Counseling Skills
Non-criticalAcceptance
- The tendency to believe generally positive or flattering
descriptions of oneself.
– An accepting attitude involves respecting clients as
separate human being with right to their own thought and
feelings. Though an accepting attitude involves
respecting others as separate and unique human beings,
this does not mean that you agree with everything they
say. It is just that you respect their version of reality.
91.
Basic Counseling Skills
Reflectingback
– Reflecting is showing the client that you have not only
heard what is being said, but what feelings and emotions
the client is experiencing while sharing his story.
- It is like holding up a mirror to the client, repeating what
they have said.
- It also allows the client to make sure your fully
understood them, and if not, the client can correct you.
92.
Basic Counseling Skills
Summarizingand checking
- In summarization, the counsellor combines 2 or
more of the client’s thoughts, feelings or behaviours
into a general theme.
- Summarization is usually used as a skill during
choice points of a counselling interview in which the
counsellor wants to draw connection between two or
more topics.
- Summarization is also used as a way to close a
session.
93.
Basic Counseling Skills
Confrontation
-Generally this means challenging the person
over a discrepancy or disagreement. However,
Confrontation as a counselling skill is an attempt
by the counsellor to gently bring about
awareness in the client of something that they
may have overlooked or avoided.
- this can be an effective response when an
issue is being denied of has not come out into
the open.
94.
Basic Counseling Skills
Challenging
-Is bringing into focus discrepancies in the other
person’s feelings, thinking of behaviour that they
tend to overlook or ignore. In the words of Fritz
Perls (founder of Gestalt therapy) “ the neurotic
is the person who is unable to see the obvious”..
Where our blind spots and distortions differ, we
are in a position to feedback to them
discrepancies that we notice from our
perspective.
95.
Basic Counseling Skills
Immediacy
–Is the ability of the counsellor to use the
immediate situation to invite the client to look at
what is going on between them in the
relationship.
It implies the use of the present tense BEING
immediate, being able to respond at the moment.
This is an essential skill needed by the
counsellor and is valuable in helping identify
feelings. It focuses on using the Here and Now.
96.
Basic Counseling Skills
GoalSetting – a very powerful tool for all areas
of Life. Hill (1975) emphasizes that establishing
goals is crucial in providing direction. Rule
(1982) states that goals are the emerging fabric
of daily living but are often elusive.
Avoidance of Judging and Moralistic
Response - The common mistake of any
person who are dealing with people through
counselling is Judging and Moralizing. Often, a
counsellor has a tendency to think that he/she
knows better and can think many possible ways
to help people with their problematic situation.
97.
Basic Counseling Skills
Theability to Offer Feedback
– Feedback is a useful tool in indicating when
things are going in the right direction or for
redirecting problem performance.
Your objective in giving feedback is to provide
guidance by supplying information in a useful
manner, either to support effective behaviour, or
to guide someone back on track toward
successful performance.
98.
Basic Counseling Skills
Workingwith Defenses
– Defenses and resistances are seen as natural
ways of avoiding discomfort, anxiety and threat
in practice. Using some counselling skills can
lower resistance and build a more cooperative
relationship.
Strengths-based Counseling of
Saleeby(1996)
The strengths perspective is not a theory — although developments in that
direction become bolder (Rapp, 1996). It is a way of thinking about what you do
and with whom you do it. It takes an ecological systems approach to problem
solving, considering social, political and cultural, as well as individual, accounts of
human predicaments and possibilities, focusing not on deficits but on the
resourcefulness of others.
101.
Strengths-based Counseling of
Saleeby(1996)
The key terms relevant to the approach are:
• empowerment;
• membership;
• resilience;
• healing and wholeness;
• dialogue and collaboration;
102.
Strengths-based Counseling of
Saleeby(1996)
The principles are:
• Every individual, group family and community has strengths.
• Trauma and abuse, illness and struggle may be injurious but they may
sources of challenges and opportunities.
• We best serve clients by collaborating with them.
• Every environment is full of resources.
103.
Gender Responsive Counseling
Emphasizesprocesses in increasing the awareness of the social order of
gender. It is occupational counselling that identifies and acknowledges
gendered structures and processes in society, as well as how they affect
men and women’s lives (Juutilainen 2003.)
It foster environment where people of all genders feel safe and empowered
so they can develop coping skills while also building a more stable sense
of personal identity.
104.
Gender Responsive Counseling
KeyConcepts:
Gender
- Refers to the array of socially constructed roles and relationships,
personality traits, attitudes, behaviors, values, relative power and
influence that society ascribes to the two sexes on a differential basis.
Sex
- Refers to the biological characteristics that define humans as female or
male
105.
Gender Responsive Counseling
KeyConcepts:
Regardless of gender identity, everyone has inherent worth and dignity and
fundamental human rights. As such, all should be treated with respect and
non-discrimination.
Gender Sensitive language
- Gender as socially stratified is evident in language, both oral and written.
- It shapes and reflects the way we think of and relate towards people.
106.
Gender Responsive Counseling
KeyConcepts:
Principles of gender fair language
- Respect for the inherent dignity, worth and rights of all people.
- Inclusiveness
- Gender equality
Guidelines for gender language
- The use of “man” refers to all human beings reinforces the invisibility of
women.
- Replace with “person” or “ human being” or their plural for,
- “he” ceases to be the universal pronoun. Replace with “she or he” or “he
and she”
107.
Gender Responsive Counseling
KeyConcepts:
Guidelines for gender language
- Use parallel language when you refer to men and women at the same
time. Examples: a. replace ‘man and wife” with husband and wife
- The order of your words should reflect your stand for gender equality.
- Refrain from using feminine endearments. Use same generic noun for
males and females.
- Do not use lady, woman or female as an adjective, in lady doctor, woman
solicitor, woman driver, or female secretary of state-unless gender
relevant” (Wright, 2003).
108.
Feminist Counseling
Feminist counselingencompasses many strands and is derived from feminist philosophy, and
feminist therapy framework.
Those women, who collectively contributed to the movement, realized that the social, cultural
and political context of their lives had to be recognized as factors in the cause of many of their
problems.
Before the emergence of feminism and feminist therapy, most women’s problems were believed
to stem from personal or innate inadequacies, usually located in the female psyche, or in
women’s refusal to conform to a predetermined and male view of how they should behave.
109.
Feminist Counseling
Clients arenot expected to adjust to a particular situation (often toxic or
abusive) but are supported in their efforts to identify personal strengths and
to change the environment that has negative impacts on them.
Feminist counsellors also acknowledge the power balance between
themselves and their clients and endeavor to encourage equality with them.
One way of achieving this is through counsellor self-disclosure and through
educating clients about the therapy process itself.
110.
LGBTQIA+ Counseling
LGBTQIA+ counselingis for adults and adolescents (ages 10-17 who have
the consent of a parent or guardian). It can also be given to spouse,
partner, family member, or other loved one struggling with concerns related
to their gender or sexuality such as having difficulty understanding or
accepting gender or sexuality. It allows client to learn positive coping skills
to help navigate the challenges they faced.
111.
LGBTQIA+ Counseling
This canhelp in dealing with a range of challenges including:
Exploring identity/orientation
Coming out
Depression
Anxiety
Gender Dysphoria
Relationship Issues
112.
Counseling for PeopleLiving with HIV
- Counseling incorporates a process of empowerment for PLHIV. It primarily
serves to prevent re-infection and provides basic information about HIV
infection, opportunistic infections and means of transmission. It also
delivers specific information on risk reduction by changing risk behaviors
(safe-sex, safe syringes, and safe motherhood). This teaches clients on
how to tell others that one is positive and handling hostility – fear & feeling
about having HIV.
113.
Counseling for PeopleLiving with HIV
- This involves establishing a supportive network to provide physical and
emotional care during the course of the disease and exploring the ways of
taking care of survivors.
- Accepting fear of death and continue to provide emotional support
- Supporting the process of anticipatory grief
- Planning continued involvement of client in self care
114.
Brief Counseling (non-crisis)
-A type of counseling that is time-limited and present-oriented.
- Brief therapy focuses on the client’s presenting symptoms and current life
circumstances, and it emphasizes the strengths and resources of the client
- The counselor in this type is active and directive. Termination of
counseling is a major focus from the initial session
Types:
• Single session Therapy
• Cognitive-Behavioral Brief Therapy
• Short-term Dynamic Psychotherapy
• Gestalt Brief therapy
115.
Grief Counseling (crisis)
Theshock and pain of loss can involve waves of feelings and sensations
that seem outside of our control. Beyond sadness, grief may manifest in
many ways such as:
Emotional
Shock, disbelief, and denial that the loss has occurred or will occur.
Anger and resentment
Regret, guilt, and shame
Depression, numbness, and feelings of emptiness
116.
Grief Counseling (crisis)
Theshock and pain of loss can involve waves of feelings and sensations
that seem outside of our control. Beyond sadness, grief may manifest in
many ways such as:
Physical
Fatigue
Nausea or loss of appetite
Heart Palpitations
Insomnia
Frequent episode of crying
Significant weight loss or gain
117.
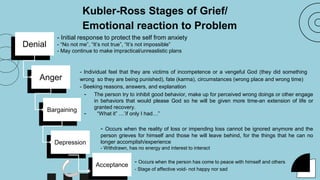
Kubler-Ross Stages ofGrief/
Emotional reaction to Problem
Denial
- Individual feel that they are victims of incompetence or a vengeful God (they did something
wrong so they are being punished), fate (karma), circumstances (wrong place and wrong time)
- Seeking reasons, answers, and explanation
- Initial response to protect the self from anxiety
- “No not me”, “It’s not true”, “It’s not impossible”
- May continue to make impractical/unreaslistic plans
Anger
Bargaining
Depression
- Occurs when the person has come to peace with himself and others
- Stage of affective void- not happy nor sad
Acceptance
- The person try to inhibit good behavior, make up for perceived wrong doings or other engage
in behaviors that would please God so he will be given more time-an extension of life or
granted recovery.
- “What it” …’if only I had…”
- Occurs when the reality of loss or impending loss cannot be ignored anymore and the
person grieves for himself and those he will leave behind, for the things that he can no
longer accomplish/experience
- Withdrawn, has no energy and interest to interact
Is a therapyapproach that focuses on
managing irrational or unhealthy thoughts,
emotions, and behaviors.
REBT focuses on actions together with a
therapist. It helps patients to identify and
dismantle unhealthy thought patterns and
behaviors.
Proponent: Albert Ellis 1950’s
Rational Emotive Behavior Therapy (REBT)
120.
How Does RationalEmotive Behavior Therapy
Work?
According to REBT, our cognition, emotions, and behavior
are connected. In order to understand the impact of events
and situations that people encounter throughout life, it’s
essential to look at the beliefs people hold about these
experiences and the emotions that arise as a result of
those beliefs.
Rational Emotive Behavior Therapy (REBT)
121.
Rational emotive behaviortherapy operates under a few main beliefs:
1. You are worthy of self-acceptance no matter what even when you
struggle or make mistakes; there is no need for shame or guilt.
2. Others are also worthy of acceptance, even when their behavior
involves something that you don’t like.
3. Negative things will sometimes happen in life, and that doesn’t mean
that things are happening in a way they shouldn’t be.
Life is not positive all of the time, and there’s no rational reason to
expect it to be.
Rational Emotive Behavior Therapy (REBT)
122.
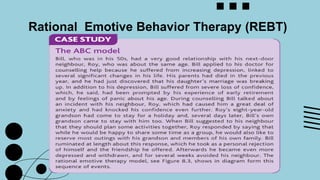
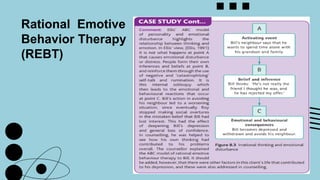
ABC Model
This modelexplains how, while we may blame external events for
our unhappiness, it is our interpretation of these events that truly lies
at the heart of our psychological distress.
"ABC" is an acronym for:
A: Activating event, which is when something happens in
the environment around you
B: Belief, which describes your thoughts about the event
or situation
C: Consequence, which is your emotional response to
your belief
Rational Emotive Behavior Therapy (REBT)
123.
Techniques
Disputation
One step towardchanging your beliefs is undergoing a process
called disputation. During disputation, worker will challenge client’s
irrational beliefs using direct methods. They may question your
beliefs head-on, causing you to rethink them, or they could ask you
to imagine another point of view that you haven’t considered before.
Ellis suggested that rather than simply being warm and supportive,
therapists need to be blunt, honest, and logical in order to push
people toward changing their thoughts and behaviors.
Rational Emotive Behavior Therapy (REBT)
124.
Techniques
Targeting Emotional Responses
WhileREBT uses cognitive strategies, it focuses on
emotions and behaviors as well. In addition to identifying
and disputing irrational beliefs, therapists and clients also
work together to target the emotional responses that
accompany problematic thoughts.
Techniques that might be encouraged include:
Meditation
Journaling
Guided imagery.
Rational Emotive Behavior Therapy (REBT)
125.
Conditions REBT CanHelp With
REBT has some data to support its benefit for a
variety of conditions, including:
Anxiety and distress
Depression
Disruptive behavior in children
Obsessive-compulsive disorder (OCD)
Social anxiety disorder
Psychotic symptoms
Rational Emotive Behavior Therapy (REBT)
Play has beendescribed as a form of self-
therapy for children. Through play, children
have the opportunity to work through conflicts,
relieve anxieties, and make sense of their
worlds. Consequently, play functions well as a
facilitative force in children’s therapy. A goal of
play therapy is to help disturbed children work
through their issues, so they can experience
pleasurable play again.
Play Therapy
129.
Play therapy canbe defined as a cluster of
theory-driven treatment modalities used to
establish an inter-personal process wherein
trained play therapists help clients prevent or
resolve psychosocial difficulties, facilitate
optimal development, and reestablish the ability
to engage in adaptive play behavior.
Play Therapy
130.
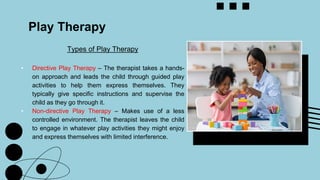
Types of PlayTherapy
• Directive Play Therapy – The therapist takes a hands-
on approach and leads the child through guided play
activities to help them express themselves. They
typically give specific instructions and supervise the
child as they go through it.
• Non-directive Play Therapy – Makes use of a less
controlled environment. The therapist leaves the child
to engage in whatever play activities they might enjoy
and express themselves with limited interference.
Play Therapy
131.
Play Therapy
Techniques
This dependson what the child needs and what play mediums they
feel most comfortable using
Using building blocks
Using Art
Sand Play
Board Games
Play with dolls
Puppet play
Tea Party Play
Card Games
Hide-and-Seek
LEGO Play
133.
Play Therapy
Case Sample
Psychiatrist:That car did something bad and now he’s no longer a car. (The child seems to be escalating in
anger at this point. He starts to crush all the cars and turn them into balls of Play-Doh.) The family of cars is all
gone now.
Mike: Yeah, now they are all bombs. I’m going to blow up this place.
Psychiatrist: The family of cars has turned into weapons. You want to blow up this building with them. (The
therapist tracks his behavior and allows him to show his anger.)
Mike: I’m going to blow you up. (He starts to throw the Play-doh balls at the therapist.)
Psychiatrist: I know you would like to blow me up by throwing those bombs at me. (This comment demonstrates
the psychiatrist’s empathy with the child.) But you may not throw things at me. You may throw those bombs at
that stuffed bear. (The psychiatrist points to a large bear sitting in the corner of the room.)
134.
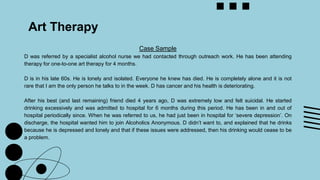
Art Therapy
Art therapycombines the process of art making
(drawing, painting, sculpture, and other art media) with
methods of psychotherapy to improve and enhance the
psychological well-being of individuals of all ages.
It is based on the belief that the creative process
involved in artistic self-expression helps people to
resolve psychological problems, develop interpersonal
skills, manage behavior, reduce stress, increase self-
esteem and self-awareness, and achieve insight.
135.
Art Therapy
Individuals whoare referred for art therapy need not
have previous experience or skill in art, because art
therapy is not primarily concerned with formulating an
aesthetic or diagnostic assessment of the people’s
images.
The overall goal of art therapy is to enable clients to
achieve emotional, interpersonal, or cognitive growth
through specific art-making experiences.
136.
Art Therapy
Aspects ofArt Therapy that makes it unique from
other therapies:
1. It helps individuals to externalize feelings and
thoughts in a unique and tangible way;
2. It helps individuals to convey feelings or thoughts
that may be difficult to verbalize; and
3. It is usually perceived as nonthreatening, neutral,
or even as “play,” reducing resistance to
treatment.
137.
Art Therapy
Case Sample
Dwas referred by a specialist alcohol nurse we had contacted through outreach work. He has been attending
therapy for one-to-one art therapy for 4 months.
D is in his late 60s. He is lonely and isolated. Everyone he knew has died. He is completely alone and it is not
rare that I am the only person he talks to in the week. D has cancer and his health is deteriorating.
After his best (and last remaining) friend died 4 years ago, D was extremely low and felt suicidal. He started
drinking excessively and was admitted to hospital for 6 months during this period. He has been in and out of
hospital periodically since. When he was referred to us, he had just been in hospital for ‘severe depression’. On
discharge, the hospital wanted him to join Alcoholics Anonymous. D didn’t want to, and explained that he drinks
because he is depressed and lonely and that if these issues were addressed, then his drinking would cease to be
a problem.
138.
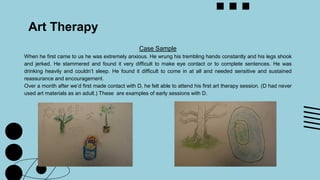
Art Therapy
Case Sample
Whenhe first came to us he was extremely anxious. He wrung his trembling hands constantly and his legs shook
and jerked. He stammered and found it very difficult to make eye contact or to complete sentences. He was
drinking heavily and couldn’t sleep. He found it difficult to come in at all and needed sensitive and sustained
reassurance and encouragement.
Over a month after we’d first made contact with D, he felt able to attend his first art therapy session. (D had never
used art materials as an adult.) These are examples of early sessions with D.
139.
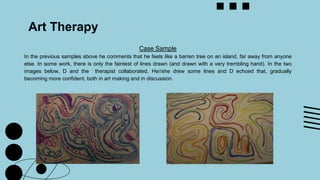
Art Therapy
Case Sample
Inthe previous samples above he comments that he feels like a barren tree on an island, far away from anyone
else. In some work, there is only the faintest of lines drawn (and drawn with a very trembling hand). In the two
images below, D and the therapist collaborated. He//she drew some lines and D echoed that, gradually
becoming more confident, both in art making and in discussion.
140.
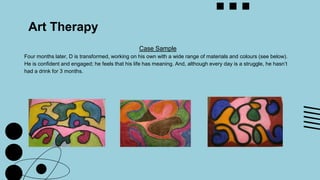
Art Therapy
Case Sample
Fourmonths later, D is transformed, working on his own with a wide range of materials and colours (see below).
He is confident and engaged; he feels that his life has meaning. And, although every day is a struggle, he hasn’t
had a drink for 3 months.
141.
Art Therapy
Case Sample
D’stransformation, his new self-confidence, engagement with life and discovery of personal strengths and
creativity (indeed, his flowering as an individual) is strikingly illustrated in his art work made in art therapy. I
believe that the experience of being witnessed is the key to D’s transformation.
D has moved from one-to-one work, to working within one of the art therapy groups. He has also started to attend
another, non-therapy group, and to make friends to other Claremont members.
D has agreed for us to show his art work. The work made in art therapy is confidential and not made for display. I
am sure you’ll respect the privilege of viewing his work, as I respect the privilege and responsibility of working
closely with individuals in therapy. This material may not be published further.
142.
Dance/Movement Therapy (DMT)
Thepsychotherapeutic kind uses body movement to promote
emotional, social, cognitive, and physical integration.
DMT can help people with physical health by increasing strength,
improving flexibility, decreasing muscle tension, and boosting
coordination. It can also offer important mental health benefits
including stress reduction and even symptom relief from
conditions such as anxiety and depression.
“DMT is a creative art psychotherapy that utilizes
movement and dance to support the physical,
intellectual, and emotional health of an individual,”
-Katie Bohn, LPC, BC-DMT,
SEP, RYT, a board-certified
dance/movement therapist.
143.
Dance/Movement Therapy (DMT)
Danceand movement therapy can be used to treat a number of
physical and mental health issues. It can be helpful for
improving self-esteem and can be useful for people who
struggle with body image issues. Some conditions that it may
help with include:
1. Anxiety
2. Arthritis
3. Chronic pain
4. Communication issues
5. Dementia
6. Depression
7. Disordered eating
8. Low self-esteem
9. Post-traumatic stress disorder (PTSD)
144.
References
● L., L.F. T., Altmaier, E. M., & Johnson, B. D. (2008). Encyclopedia of counseling (Vols. 1–
4). SAGE.
● Seden, J. (2005). Counselling skills in social work practice [PDF] (2nd ed.). Open
University Press.
● Hough, M. (2014). Counselling skills and theory [PDF] (4th ed.). Hodder Education.
● Corey, G. (2009). Theory and Practice of Counseling and Psychotherapy (8th ed., pp.
339-369). Belmont, CA: Thomson Brooks/Cole.
● Feminist Therapy - Approach. (n.d.). In American Psychological Association. Retrieved
from http://www.apa.org/pubs/videos/4310828.aspx?tab=2
● https://us.sagepub.com/sites/default/files/upm-assets/4991_book_item_4991.pdf
● https://cswcd.upd.edu.ph/wp-content/uploads/2022/10/CDJ-1997_Whole-Book.pdf










![References
● L., L. F. T., Altmaier, E. M., & Johnson, B. D. (2008). Encyclopedia of counseling (Vols. 1–
4). SAGE.
● Seden, J. (2005). Counselling skills in social work practice [PDF] (2nd ed.). Open
University Press.
● Hough, M. (2014). Counselling skills and theory [PDF] (4th ed.). Hodder Education.
● Corey, G. (2009). Theory and Practice of Counseling and Psychotherapy (8th ed., pp.
339-369). Belmont, CA: Thomson Brooks/Cole.
● Feminist Therapy - Approach. (n.d.). In American Psychological Association. Retrieved
from http://www.apa.org/pubs/videos/4310828.aspx?tab=2
● https://us.sagepub.com/sites/default/files/upm-assets/4991_book_item_4991.pdf
● https://cswcd.upd.edu.ph/wp-content/uploads/2022/10/CDJ-1997_Whole-Book.pdf](https://image.slidesharecdn.com/sw-counseling-presentation1-250719030116-3895eec3/85/SW-COUNSELING-PRESENTATION-1-pdf-SWSWS-144-320.jpg)