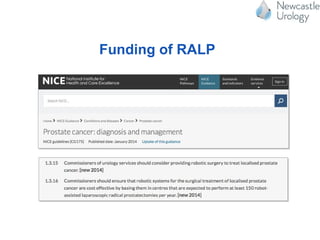
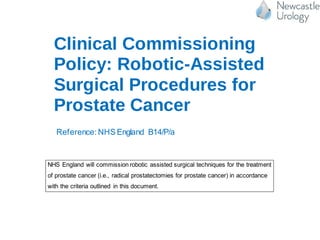
The document discusses robotic surgery services in the UK. It notes there are around 50 robots currently in the UK, with most located in southern regions and private practice. The NHS funds robotic-assisted laparoscopic prostatectomy (RALP) and robotic-assisted nephrectomy (RPN) procedures. It also discusses a clinical commissioning policy from NHS England that outlines criteria for funding robotic prostate cancer surgeries. Finally, it mentions that the Freeman Hospital in Newcastle was the first in the northeast to use a robotic surgery system and has now performed over 1,000 operations with robotic assistance across six surgical specialties.