Download as PDF, PPTX

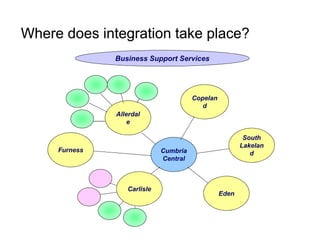
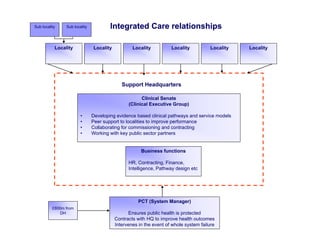



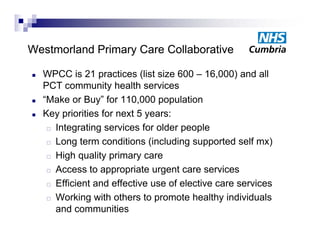
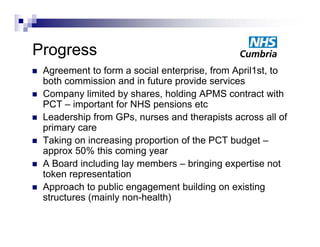
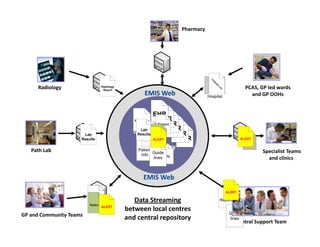
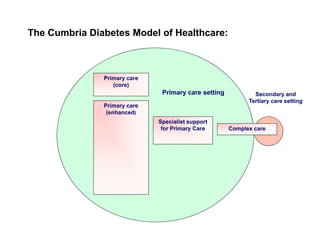
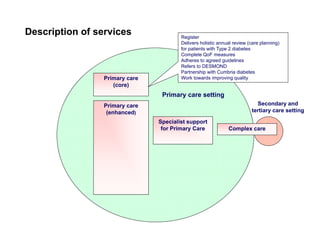
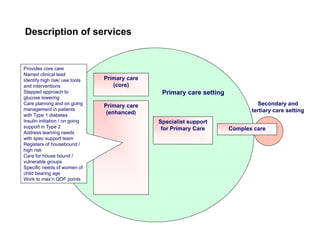
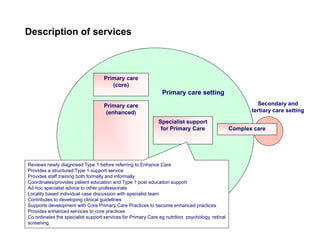
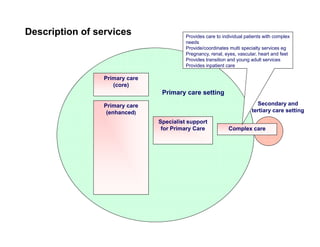
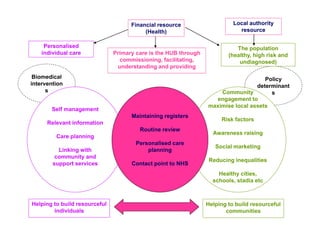
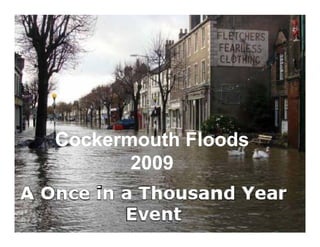
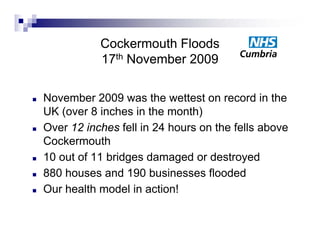

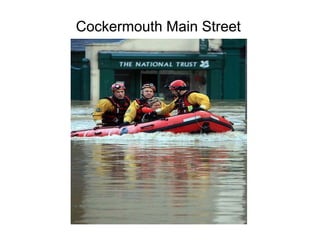
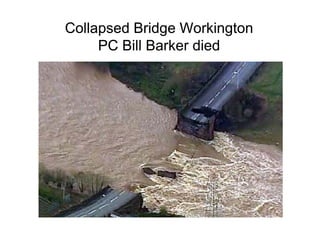


Integration in Cumbria aims to improve health outcomes through closer collaboration between primary, community, and acute care services. Key steps have included forming a social enterprise to both commission and provide community services, giving clinicians leadership roles in localities, and devolving power to integrated care organizations. This approach has helped solve a historic health economy debt, improve quality scores, and establish new models of care like the "virtual community hospital" and integrated diabetes services. The integrated system also responded effectively to the 2009 Cockermouth floods.



































































