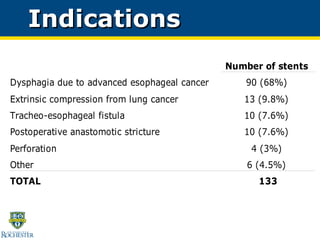
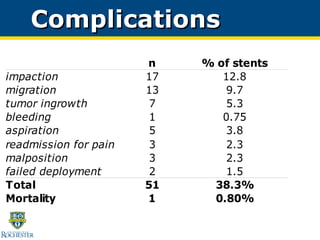
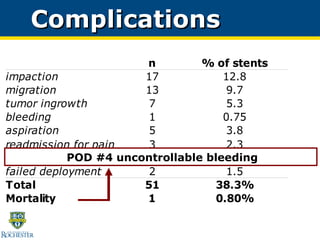
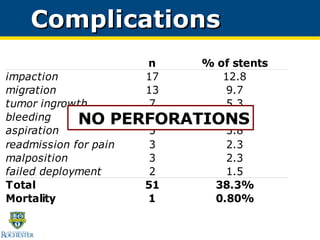
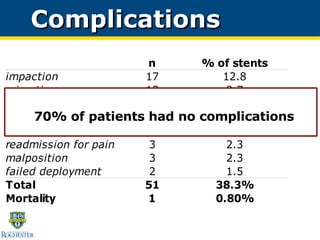
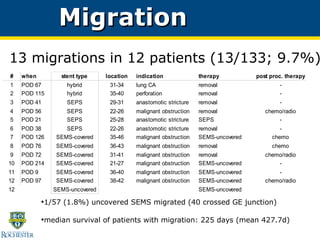
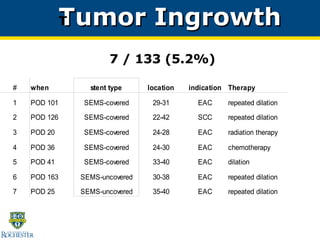
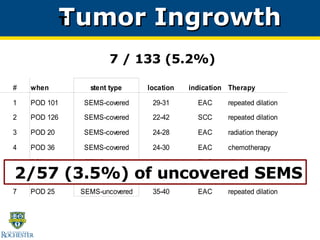
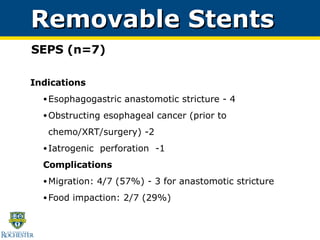
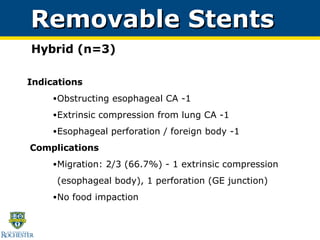
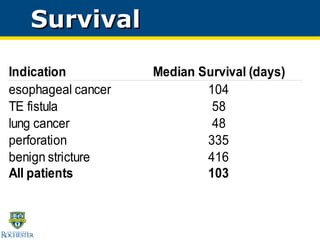
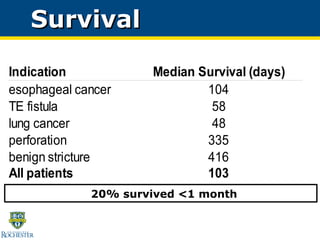
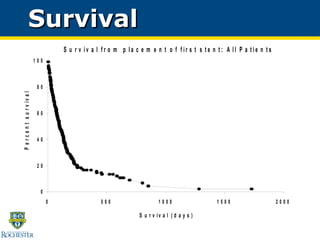
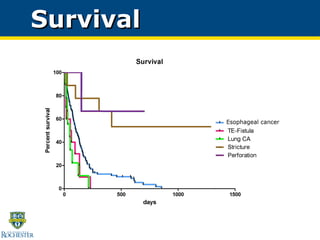
This study evaluated the use of self-expanding metal stents, plastic stents, and hybrid stents to treat 133 patients with malignant and benign esophageal diseases over an 8-year period at a single institution. Stent placement was successful in relieving obstruction in 91% of patients with a median hospital stay of 1 day. Complications included migration in 9.7% of cases, impaction in 13% requiring endoscopic disimpaction, and tumor ingrowth in 5.2% of uncovered metal stents. Stent placement was found to be a generally safe, quick, and reliable procedure for palliating malignant esophageal obstructions.








































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







